
(Part 2)
| A 38-year old transwoman after breast augmentation surgery to insert 2200cc breast implants. She is now technically a 42JJ bra size. |
During the first 24 to 48 hours after your surgery, you will experience the most discomfort. Your breasts will be swollen and very tender. Although every woman's recovery time is different, you should be able to resume many of your regular activities after about one week. You will need to wait at least one month before resuming any strenuous activities. Should any problems occur after surgery, contact your doctor immediately. This is especially important if your temperature is elevated, or one of your breasts is noticeably more swollen and tender to the touch, painful, red or inflamed. After
surgery, implants will ride high on the chest. It will normally
take 4-12 weeks for them to "drop" into place. The more natural
breast tissue you have and the smaller the implant, the more natural the
look. Keep in mind, most women wish they had gone larger!
Placing them under the muscle also allows for a more natural appearance.
As you age, your natural breast tissue will sag, the implant will not. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
| Augmentation Complications |
3-Year Risk Rate |
|
|
By Patient |
By Implant |
|
| Wrinkling |
21% |
20% |
| Reoperation |
13% |
10% |
| Loss of Nipple Sensation |
10% |
8% |
| Capsular Contracture Grade 3/4, or grade unknown |
9% |
7% |
| Implant Removal |
8% |
6% |
|
Asymmetry |
7% |
5% |
| Intense Nipple Sensation |
5% |
4% |
| Breast Pain |
5% |
4% |
| Leakage/Deflation |
3% |
2% |
| Implant Palpability |
2% |
2% |
| Infection |
2% |
1% |
| Breast Sagging |
2% |
1% |
| Scarring Complications |
2% |
2% |
It's worth noting that more than 1 in 5 (21%) women experienced problems with wrinkling and ripples, and probably more than half experienced some form of problem, of greater or lesser significance, within 3 years of their breast augmentation. Clearly breast augmentation is still not a trouble free experience for many women, whatever some surgeons may try to imply.
 Poor quality breast implants are the bane of many attractive transwomen. Of course the cost of using a top surgeon is often the reason. |
Over half of all transsexual women eventually have breast augmentation and the results are well documented. It's informative to quote the results of one survey here to see if the pain, expense and complications are all considered worth it by transsexual women ...
One hundred and seven post-operative male-to-female transsexual woman were surveyed an average 5.5 years after mammaplasty (range, 16 months-17 years. The age of the woman ranged from 22 to 76 years (average, 41 years). Seventeen of the 107 women had undergone further augmentation mammaplasty, on average 57 months after the initial mammaplasty. The average size of implanted prostheses was 258 ml (range, 130- 450 ml).
A good result using the periareolar methodEighty women (75%) indicated satisfaction with the final outcome of the mammaplasty. The median postoperative cup size in this group was B (range of postoperative bra size, 30B-40D).
The remaining 27 women (25%) were unhappy with the results of mammaplasty. The median postoperative cup size in the 18 women who still felt their breasts to be too small was also B (range of bra size, 30B-48E). The average size of current prostheses in these 18 women was 261 ml.
It's notable that despite the desire of many transsexual women for large breasts, the two women with an augmented 40D and 48E bra size are clearly exceptional. The most common result is a moderate B cup and the average implant size is an also moderate 260ml, the largest being only 450ml. This, and the relatively high percentage of women feeling that their breasts were still too small, is unfortunately an indication of the limitations imposed on augmentation by the small natural breasts typical of pre-augmentation transsexual women. See the at the bottom of this page photo of an augmentation by the famous surgeon Dr. Douglas Ousterhout as a demonstration that even the best surgeon can only achieve so much with the material they have to work with.

(Above) Despite multiple challenges, the surgeon has achieved excellent results for this transwoman.

(Above) Another procedure performed by same surgeon, the
results are still good but the nipples are
positioned slightly too
high and their surrounding areola have not stretched.
When any type of breast implant is inserted, the body's immune system reacts by forming a protective lining made from collagen around it to protect itself from this foreign body. This is referred to as the "capsule" or "tissue capsule."
The formation of a capsule is normal and happens in everyone regardless of whether the implant is smooth or textured, silicone or saline. Under ideal circumstances, the capsule maintains its original dimensions and the implant rests inside it, remaining soft and natural appearing. However, for reasons that are unknown, in some women the capsule has a tendency to shrink, squeezing the implant. An implant that is compressed hardens like a balloon, i.e. the tighter the capsule becomes the firmer the breast feels. This problem is called "Spherical Capsular Contracture". It has been known since the very early days of implants and has always been considered to be the main problem with breast implants.
 Transwomen can seek very different appearances from their breast augmentation surgery. |
The degree of capsular contracture is measured on the "Baker Scale", from grade 1 to 4. Grade 1 means the breast looks and feels so soft that the capsule is virtually undetectable; while Grade 4 means the implant is painful and as firm as a grapefruit, and that it is being distorted in shape and squeezed out of position.
No matter the degree of capsular contracture, it is not the implant that gets hard, if the implant is removed it is as soft as when it was inserted, it is the interaction of the capsule with the implant that makes the breast feel firm. Capsular contracture alone does not cause implant rupture because the force is exerted evenly around the surface of the implant.
Encapsulation may occur immediately after surgery or many years later, and may occur on one or on both sides. The incidence of capsular contracture approached 100% in the 1970s, subsequent modifications in implant design and the surgical procedure have reduced this undesirable effect significantly, according to various studies and surgeons claims, the frequency of significant encapsulation (Grade 3 or 4) among women with saline-filled breast implants currently ranges anywhere from 5 to 18%.
It should be noted that a mild to moderate degree of contraction usually. Most encapsulation is of a mild degree (Grade 1 or 2) that doesn't detract from the quality of the augmentation result and is not considered clinically significant. Indeed, for some women a mild degree of firmness in their breasts, similar to a pubescent girl's, may actually represent a desirable outcome.
The treatment of severe capsular contracture is usually surgical. In an "open capsulectomy" the surgeon scores, or cuts, the capsule to release its hold on the implant. In a "closed capsulectomy," the entire capsule is surgically removed. The body then forms a new capsule but the hope is that it does not contract as the old one did. Capsulectomy is a more extensive operation than capsulotomy but has a higher rate of success in correcting contracture. Only a relatively small percentage of women with implants develop capsular contracture severe enough to require surgical treatment. The rare patient develops repeated capsular contracture but in the majority of cases it can be successfully treated.
Some transsexual women insist on choosing excessively large and inappropriately shaped implants for their available breast tissue coverage in an unrealistic desire to achieve "Playboy" breasts. At best its very obvious that they've had breast implants, whilst in the very worst cases the implant can actually start to emerge through a hole in the skin at the bottom of the breast.
The most common visible problem with overly large breast implants is traction rippling. Rippling looks like someone had their fingers on the breast and left indentations, it is not a permanent rippling in most cases but a ripple occasionally as the implant moves and literally ripples, giving the skin a wave-like appearance instead of the smoothness you see in a normal breast. When you spot an actresses or lingerie model with obvious and over large implants, then you have probably seen this phenomenon. Some 20% of genetic women with implants experience problems with rippling, and the incidence is probably even higher in transsexual women who tend to over size their implants.
 |
Age: 30, Height: 5'5", Weight:
115 lbs Implants: 700cc filled to 780cc, textured, saline Placement: Submuscular, with periareolar incision |
|
(Above) An example of severe implant malposition, drop-out of the inframammary creases, severe bottoming out, and obvious traction wrinkling. The problems are all due to much too large a size implant, with a textured shell, in a woman with little body fat (i.e. thin!) and inadequate soft breast tissue coverage. |
|
Every breast implant has at least a little bit of wrinkling, an irregularity of its surface. Some implants have very little, and some have a lot of it; if there is little, then it may not even be detectable. If there is more, it may be felt, and if there is a lot of wrinkling, then it can be felt and even seen as rippling. In general, the degree of wrinkling depends upon several factors that work to either hide or reveal wrinkling or rippling. The areas where rippling is usually most apparent are the outer side near the arm, along the bottom, and towards the cleavage, in that order. The rippling is most objectionable when it is visible at the top of the breast. For that reason, placing implants beneath the large pectoral muscle can be particularly advantageous with saline implants. The thickness of the muscle obscures whatever wrinkling there might be, in the same way that a thick carpet will hide uneven floor boards.
 Age: 40, Height: 5'7 ", Weight: 110 lbs Implants: 370cc, smooth, saline Bra Cup Size: 36 C Note: Implant displacement and severe bottoming-out, again caused by overlarge implants for a thin woman with minimal natural breast tissue. |
Saline implants tend to ripple more than silicone gel or other materials.
It is in the nature of saline inflatable implants to have wrinkling of
the shell. This is because the shell needs to be thick and strong
enough to last as long as possible, and because the saline (salt water)
fill shifts with changes in body position. In addition, if a
saline implant is not filled up to the optimum, which may require
overfill, there can be rippling at the top of the breast also.
Every saline implant has an optimum volume of saline fill, a volume that
gives the best balance between either wrinkling (caused by not enough
saline) or too firm/round (caused by too much saline). The
difference between inadequate volume and the optimum volume is
astonishingly small, around 10%, which may be only a couple tablespoons
of water! Women who are troubled with rippling because their
implants were not filled to the ideal optimal volume may need an
operation to add that critical tablespoonful of saltwater that makes all
the difference.
 Lorna, a 24 year old transwoman before and after 425cc "Gummy Bear Bear" implants. She is very happy with the result. |
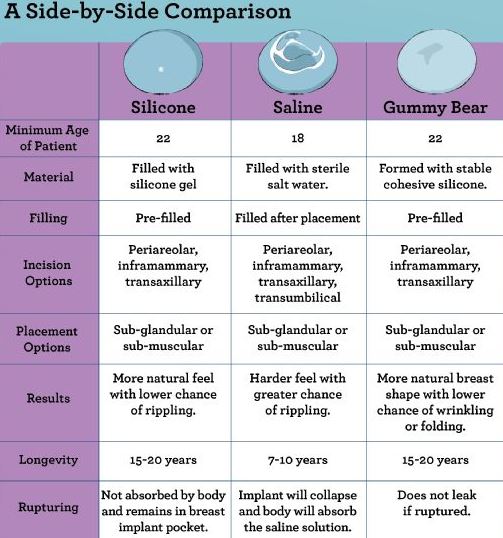
Gummy Bear
A development since this article was originally written in 2001 has been the emergence and approval by medical authorities of so-called "gummy bear" implants. These are highly cohesive silicone gel breast implants - with the implication being that there is no containing envelope like traditional silicone or saline implants, and that the whole implant is effectively a jelly-like silicone compound that can't burst or leak. Post surgery it is difficult to tell the difference between traditional silicone implants and a "gummy bear", but the manufactures claim that it can't rupture is already disputed by patients.
 These transsexual women demonstrate a look all too common - solid, unnatural, widely spaced, semi-spherical breasts stuck on to the chest. This occurs when over-large implants are inserted under a minimal amount of natural breast tissue, often prematurely, i.e. before maximum possible amount of hormone induced development.
|
Despite the every effort of implant manufacturer's and surgeons, the look and feel of breasts with implants will be different (to some degree) from that of similar size real breasts. Have you ever paged through a lingerie catalogue and been sure that one of the models had breast implants? Well, that's probably because implants can make the breast look unnaturally rounded. Most implants are half spheres in appearance while natural breast shapes are more parabolic or U-shaped. Women with large implants may also get a "double breast." This is because the normal breast hangs, but the implants stick straight out from the chest wall. This makes the breast look like it has a hump in the middle when looking at it from the side. When pushed up, the implants' upper border will show through the skin. Two deeply curved upside down lines get etched in the skin. When pushed together, well... they don't push together. It is like putting too balls together; they meet in the middle and leave a gap on either side. This is in contrast to the straight line formed by natural breasts. When left alone, implants leave a flat valley-like gap where the breastbone (the sternum) is, between the implants. Natural breasts slope more gradually towards the centre.
Measure's can be taken to minimise and reduce all these problems, but they cannot be completely eliminated with the current breast augmentation technology.
 The
Feel
The
FeelWhen doctors say that implants feel the same as normal breasts, they are talking about how they feel to others touching the breasts, not about how they feel to the woman with the implants. Implants can make it harder to sleep on your stomach and they often feel cold. Silicone gel and plant oil-filled breasts have a good reputation for feeling comfortable and natural to the woman, but saline-filled implants don't have the same density as tissue so the weight of the breast feels odd for its size.
The body forms capsule tissue around the implants, in some women this causes the breasts to feel artificially firm or even hard.
The difference in the feel of the breasts can also have an impact on cancer screening. If the augmented breast does not feel the same as the natural breast, it can be difficult to determine if there is a change in the breast that should be checked out. Also, there are changes that will occur in the breast due to the implant that will have nothing to do with cancer, but these changes can cause alarm when they are first noticed.
|
|
Give-away's caused by over-large implants or other factors (including poor quality surgery) include:
Factors that increase implant give-aways:
Factors that decrease implant give-aways:
Transsexual women who "pass" successfully have usually taken the advice of their surgeon and settled for appropriately shaped small-to-medium implants which give them natural appearing augmented breasts of perfectly adequate size for their build.
|
|
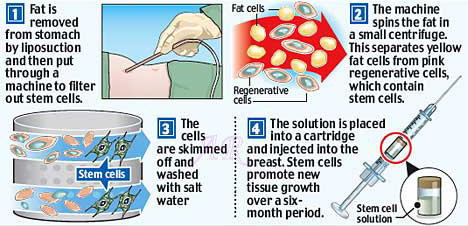
The last decade has seen the emergence of a solution for transwomen who want to increase the size of their hormone induced breasts by a modest amount without surgery.
The procedure involves injecting fat cells into the breast tissue. Fat is taken through liposuction from the woman's belly or bottom. The fat cells are filtered out from the extract and then put into a cartridge for injection into the breasts about an hour later under local anaesthetic. Some practitioners refer to the 'fat cells' as 'stem cells' - technically this is correct although their ability (potency) to differentiate into different cell types is low and the claimed six months of subsequent breast growth in the diagram below is very dubious.
![]()
Realistially there is an immediate substantial increase in breast volume after the injection of the fat cells into the breasts, but about 30% of the gain is lost within a few weeks, and the long-term loss is typically 50-70%. Nevertheless, it's a good option if a quick and confidence boosting increase in breast size is needed, e.g. for a beach holiday, a beauty contest or even a wedding!
|
|
For transwomen with reasonable but not quite sufficient hormone induced breast development, this technique can be a good alternative to breast augmentation. It should round out their breasts and provide a modest boost in size. Importantly there are no signs of surgery and no implants to mare the feel of the breasts. Whilst the temporary stretching of the skin can result in some subsequent breast drooping - this is often desirable for middle-age transwoman seeking a natural appearance equivalent to cis-woman of a similar age.
When I wrote the first version of this article in 1999, I found a large body of medical literature dedicated to breast augmentation, but nothing specifically related to breast augmentation in transwomen - which I considered at the time to be a major gap.
I have since found several studies that consider breast augmentation in transwomen, and have added summmaries here.
Study 1
 Laura, born Darren. She has had multiple breast augmemantion procedures |
"Gender-affirmation surgery is essential in the management of gender dysphoria. For male-to-female transgender women (transwomen), feminization of the chest is a component in this process. There is minimal literature describing effective and safe techniques for breast augmentation in transwomen."
A summary of the key points and findings:
The study also noted:
The study concluded that "Breast augmentation in transwomen is safe and typically leads to high patient satisfaction with improvement of gender dysphoria".
The study included the photos below:
|
|
|
|
A transwoman having
breast augmentation surgery. (A) Preoperative markings, (B) surgical plane, (C), implant insertion, (D) on table result. |
Photos of the
same transwoman preoperative (top) and 1-year postoperative
(bottom). |
In June 2020 a study entitled "Breast Augmentation in the Transfemale Patient: Comprehensive Principles for Planning and Obtaining Ideal Results" (Coon et al) was published by the American Society of Plastic Surgeons, it can be found online here.
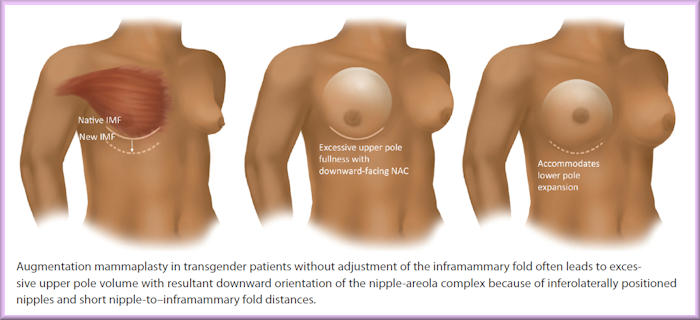
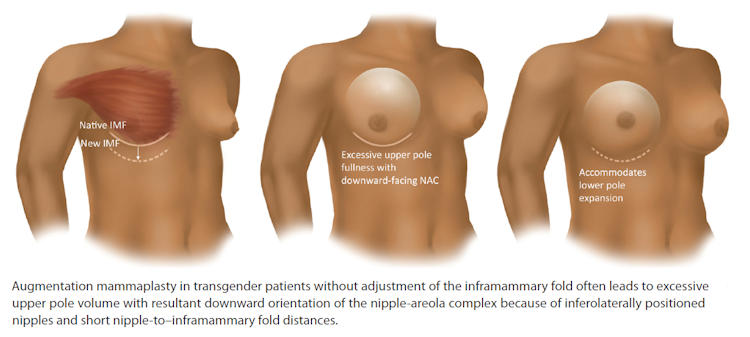
The study has several useful findings. In the 36 transwomen they studied who had undergone BA, 91.7% received a lowering of the inframammary fold - the point where the bottom of the breast tissue meets the chest. The authors emphasize the key role of this step for trans patients: “Perhaps the most critical difference to appreciate in transgender augmentation is the need for routine inframammary fold adjustment, in contrast to cosmetic mammaplasty.” Without lowering and reconstruction of the inframammary fold, the implant could be positioned too highly and cause the nipple to point downward.
In most cases, low-profile (wide diameter, less height) and high-profile (narrow diameter, greater height) implants are avoided in favor of medium-profile implants, with high-profile implants used only rarely in those few patients who have “narrow chests, substantial breast development on estrogen, and a desire for maximum size”. The authors also report that in their experience, shaped teardrop implants do not produce a visible difference compared to round implants, and carry a risk of improper positioning as well as the development of anaplastic large-cell lymphoma due to their textured surface.
Additionally, they recommend placement of implants beneath rather than above the pectoral muscle, as trans women’s breasts may have a “small diameter”, and placement directly underneath the mammary gland but atop the muscle can create the appearance of “an unnatural double mound” and “visible implant edges”. Subpectoral placement can also help avoid the outcome of an overly wide gap between the breasts, a risk for trans women with broad ribcages:
Aggressive release of the pectoralis with partial-thickness release of the thick sternal insertions (taking care not to fully release it) can help to address the problem of excessive cleavage gap from greater sternal bone width.Among the patients treated at this surgical centre, 79% reported being very satisfied with their overall cosmetic result, and 21% were moderately satisfied. Awareness of these factors can help trans women and their providers make the aesthetically optimal choice when planning an augmentation surgery. With these techniques, many of the concerns specific to trans women’s anatomy can be mitigated, resulting in a satisfying outcome that aids in the treatment of gender dysphoria.
Study 3
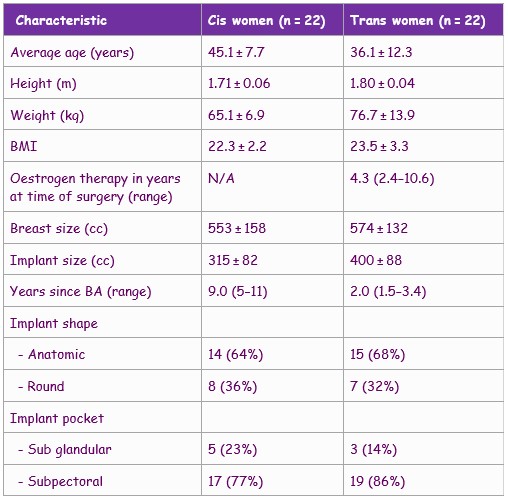
Perhaps the most relevent study to date is "An anthropometric evaluation of the augmented breast: differences between cis-and transgender women and possible clinical implications", published in the Journal of Plastic Surgery in July 2021. Available on-line.
This is essentially a simple study which compares the results of breast augmentation in 22 cis women with that of 22 trans women. To reduce variable and aid comparision, all augmentations were via the inframammary technique.
The table below shows the characteristics of the 44 women studied.
Each subject was scanned using lasers to gain accurate measurements and a 3D model of their body. The image below portrays the aggregated results for the ciswomen (left) and the transwomen (right). The depictions are to scale.
![]()
In key criteria such as breast width there was statistically little difference between the augmented breasts of cis and transwomen. However the study identified distinct structural differences. Although the implants of the transwomen were generally larger and positioned more forward facing (presumably a result of a wider chest), their nipple-areola complexes (NAC) were significantly smaller (not evidenced in the above image) and positioned relatively more side facing.
The study has a significant weakness in that the ciswomen included are much older than the transwomen, and thus most have probably had children. Nevertheless, it is clear that surgeons need to adjust their procedures for transwomen seeking breast augmentation with a final appearance similar to cis women.
 (Top) One month before BA (Below) 6 months after BA. The areolae have stretched and the breasts are equal in size, the scars (at the bottom curvature) are barely visible. Whilst biased, I think it's a good result. |
After years on hormones, my breast development got stuck at a modest 36B cup size. My boyfriend, soon fiancée, felt that my breasts were on the small size and encouraged me to have breast augmentation.
In January 2002 I visited a clinic for a consultation. This was just before computer visualisation tools appeared and I spent the most of the hour looking at photos and experimenting with bras and fillers in the two outfits that I had bought with me - as requested - in order to determine the appearance that I wanted to achieve. At the end I was advised to have pre-filled silicone implants of about 280cc, located under the muscle via a breast crease (aka inframammary) incision.
Six weeks later, whilst I was being prepared for surgery, the surgeon decided to give me round, smooth, high profile, “Paragel” silicone gel implants - 300cc on the left but 325cc on the right as this breast was slightly smaller. I wasn't in a position to debate this!
After surgery my breasts seemed far too prominent and I initially dressed very modestly. But after about six months I had become more used to their substantial size, and their appearance had greatly improved thanks to a combination of sagging and gaining some otherwise unwanted pounds. My bra size settled down to a 38D or 40C - depending on the brand.
I thankfully had no complications and to my surprise my
breasts still felt very natural and I struggled to detect the implants.
My enlarged breasts were probably ideal for my
appearance (not too big, not too small) and I rarely felt the implants
even when trying to sleep. Despite this, I was still very conscious that I
had
large blobs of silicone gel sitting in my body.

I had two of these in my body for 20 years.
In early 2020 I had a mammogramm. Whilst the results were all-clear, because of my background I was still seen by a doctor. She suggested that it was probably time to replace my aging implants, recommending anatomically shaped implants that would give my breasts an appearance more appropriate for my age when topless.
The advent of the Covid pandemic meant that it was not until 2022 that I had the implant replacement procedure. But, again, it went well and the latest generation of implants offer improvements such as a biocompatably shell that make complications unlikely. The new implants should last 20+ years, which being realistic means that they may well outlive me.
I attempt to show here a diverse range of implant results illustrative to the diverse range of procedures and implants types possible.
 |
 |
| Age:
20 Implants: 475cc, smooth, round Placement: Submuscular Bra cup size: ? |
Age:
19 Implants: 275 cc, smooth Placement: Submuscular, transaxillary incision Bra cup size: 32A to full 32B |
 |
 |
| Age:
25 Implants: 350 cc, smooth, saline Placement: Submuscular, transaxillary incission Bra cup size: AA to C |
Age:
29 Implants: 250 cc Incision: Inframammary Bra cup size: 34A to 34 C/D |
 |
 |
| Age:
19, Height: 5'7", Weight: 115 lbs. Implants: 300 cc, anatomic Incision: Transaxillary Bra cup size: ? |
Age:
25 Implants: 530 cc, round, saline Placement: Submuscular, inframammary incision Bra cup size: A to large C |
 |
 |
| Age:
24 Implants: 395 cc, smooth, round, saline Placement: Submuscular, periareolar incision Bra cup size: 34A to 34C |
Age:
26, Height 5'4", Weight: 107 lbs. Implants: 430 and 440 cc, smooth, round, Mentor Spectrum expandable Placement: Submusclar, TUBA incision Bra cup size: 34A/B, Post 34 D |
 |
 |
| Age:
19 Implants: 320 cc Incision: Transaxillary Bra cup size: 32A to 34 D |
Age:
19 Implants: 285 cc, smooth, round, saline Placement: Subgandular, inframammary incision Bra cup size: 32A to 34 C |
 |
 |
| Age:
24, Height: 5'5", Weight: 128 lbs. Implants: 475 cc, round, smooth, saline Placement: Subglandular, inframammary incision Bra cup size: 32 AA to 36 D |
Age:
29, Height: 5'3", Weight: 118 Implants: 570cc, smooth, round, Mentor Spectrum Placement: Submuscular Bra cup size: 34-36B to 34-36D |
 |
 |
| Age:
? Implants: 700 cc, silicone gel Placement: Submuscular Bra cup size: ? |
Age:
? Implants: 475 cc, round, smooth, saline Placement: Submuscular, periareolar incision Bra cup size: ? |
 |
 |
| Age:
28 Implants: 350 ml round silicone gel (Mentor plus profile) Placement: Submuscular Bra cup size: ? |
Age:
35 Implants: 300mm and 325 cc round, smooth, silicone gel Placement: Submuscular, inframammary incision Bra cup size: 36A to 38C |
Hundreds more fully documented examples of breast augmentation, including "Before and After Photos" and a lot of other useful information, can be found at the "All about Breast Augmentation and Breast Implants Resource" and Nicole's huge "Breast Augmentation & Breast Implants Information Web".
In Europe, the typical transwomen transitions in her early 30's and - after several years on hormones - has breast augmentation. The following sequence of 'before and after' photos were selected by a medical publication dated 2020 to try to show the results for the typical transwoman. Interestingly, the tattoo evidences that she almost certainly the same transwoman as in some photo's (shown further below) that I had received over a decade earlier.

The pictures below are provided by Leah. The left picture was taken soon after her breast augmentation in her late 30's. This involved a inframammary incision and the skin of breast is still very stretched and the outline of the profiled implants fairly clear. The right-hand picture is taken several years later and the breasts have settled in to a more natural looking appearance, probably aided by some additional hormone induced tissue development. The exceptionally large areolae (for a transwoman) are slightly marred by the uneven stretching and the surrounding area seems to have a slight skin rash (just visible in the photo), possibly caused by the implants being too near the surface (i.e. subglandular).

The following pictures show Larisa. An initially good impression (left) of her breast augmentation is countered (mid/right) by the implants being obvious and very unnatural in appearance when topless.

Next is Teddy Quinlivan - a female model who out'ed herself as a transwoman in 2017. As shown in the left photo, her breast development age 22 was minimal despite taking oestrogen hormones for five years. After a lot of research and very careful consideration as to how larger breasts would affect her appearance, she had round breast implants of just 100 cc. Despite the small size, the implants were initially very obvious, as seen in the inset photo. However, over the next two years they settled and she is presumably now happy with results as she regularly posts topless photos of herself on social media. The right most photo shows her age 24.

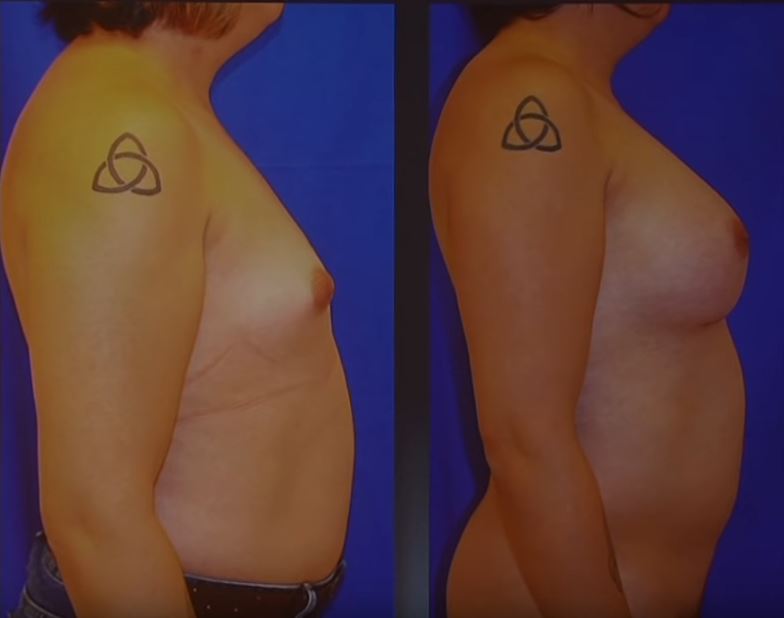
Below, before and after photos of a transgender woman who started hormones age 31 and had breast augmentation surgery age 34.

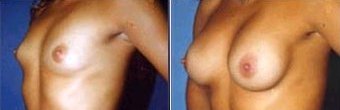
Below, before and after photos of the breast augmentation of a transgender woman published in a medical paper. She was age 24 and had taken estrogen for just 30 months before surgery.

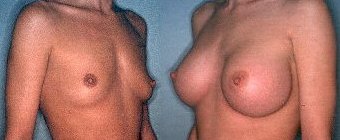
Below, before and after photos of the breast augmentation of a transgender woman published her by surgeon. He provided no details other than that she was age 25.

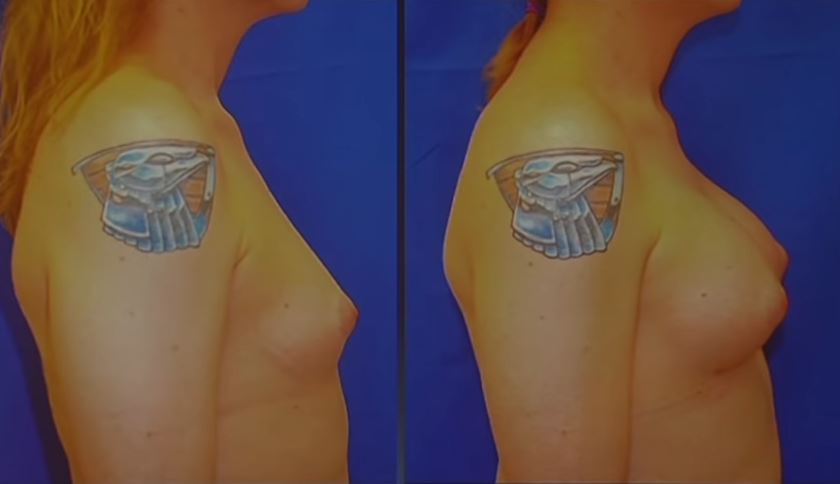
Below, before and after photos of a 27-year transwoman. The profile of the right breast has improved dramatically. Unfortunately, I have no frontal photo, which would be interesting.

27 years old
The photo below shows a middle-aged transwoman after BA with large 600cc implants. These are too large for the pre-existing breast tissue, with early signs of rippling. The outward bulging in the superior lateral (aka upper outer) quadrant of the breasts is a tell-tale sign of excessive augmentation. But if her personal goal is to be a generously endowed woman, maybe it's a success - at last for a while.

The following 'after' examples are again provided by surgeons, as such they are probably particularly good results.
|
|
| Surgeon: Dr.
Douglas Ousterhout Implants: 350cc, saline Placement: Submuscular, periareolar incisions Note: Notice the considerable distance between the breasts even with a high quality augmentation from a top surgeon |
|
|
| Surgeon: Dr
Toby Meltzer Implants: Saline, size unknown Incision: Submuscular, periareolar incision |
|
|
| Surgeon:
Dr Suporn Watanyusakul Implants: 400 cc, silicone gel Placement: Submuscular, transaxillary incision |
|
|
| Surgeon:
Dr Suporn Watanyusakul Implants: 300 cc, silicone gel Placement: Submuscular, transaxillary incision |
Below, a 24-year old transwoman after 30 months on estrogen. Shown before (A-C) and one month after (D-F) subfascial breast augmentation. Her body mass index (BMi) before surgery was a healthy 23.6.
![]()
Below, a 18-year old transwoman after 54 months on estrogen. Picture A is just before she underwent subfascial breast augmentation surgery and E-G are four months after. Her body mass index (BMi) before surgery was 35.1, so a bit over weight.
![]()
Below, 'Before and After' breast augmentation photos of four transwomen provided by a clinic. No details of the procedure were included. Note yet again the small nipples/areola that so often unfortunately distinguish the breasts of transwomen from cis women.
 |
 |
 |
 |
 |
 |
 |
 |
Finally, in 2000 I struggled to get even photos of even a dozen transwomen showing the results of their breast augmentation, relying on examples sent to me by a few on-line friends and references provided by a couple of surgeons. However, the results were often good. 25 years later the Internet is awash with photos of topless transwomen. I did a google with safe mode turned off and picked a sample of photos from women who seem to be in their 20's or 30's - i.e. will have potentially benefited from modern post-2000 BA techniques. Overall, I found the results to be very dispiriting, with a clear tendency to have excessively large implants without adequate hormone induced breast tissue.

Last updated: 1 December, 2025
|
Formerly the "Birth of Venus"
(c) 2000-2025 Annie Richards |















 Back to Articles
Back to Articles (No spaces)
(No spaces)