
In 2002 Ron Mueck
created this extraordinary larger than life statue of a "Pregnant Woman".
Twenty years later
a young British transwoman posted a photo of it on social
media with the caption: "I just want to have a baby".
|
Important Note: This article is not intended to provide any medical advice or recommendations, and I can't accept any liability for any decisions made based on its content. Please always seek qualified professional medical advice before having any treatment or procedure. Nomenclature: There is currently (2020) intense pressure from LGBTI+ activists to avoid the use of words such as 'man' and 'woman' in a sexual and reproductive context. This campaign has had great success, for example the Australia National University’s Gender Institute Handbook suggests that the word 'mother' be replaced by 'gestational parent', and 'father' by 'non-birthing parent'. In the UK, the hugely influential charity Stonewall is requiring member organisations (including schools and children's hospitals) to replace the words "boy" and "girl" with gender neutral terms such as "they". However, the first version of this article was written in 2001 using traditional nomenclature - which I'm very reluctant to change. |
|
Peer reviewed
medical papers have long concluded that there are no longer any
significant medical barriers that prevent a transwomen being given a
uterus transplant and getting pregnant. Indeed, some medical
professionals such as Dr Rebecca Flyck at the prestigious Cleveland
Clinic in Ohio
argue that not opening up this procedure to transwomen is a form of
discrimination. But as of 2026, there seems little likelihood that
this will happen in the foreseeable future.
Medical opinion has unfortunately reached a consensus that there are
serious ethical and legal issues that need to be resolved before
transwomen can become eligible for a uterine transplantation. As a
result, the 2012
Montreal Criteria advised that such
transplants should only be offered to "genetically female" and natural
born women. Some specialist teams working in the field, e.g.
Womb Transplant UK, take this even
further and refuse to even conduct supporting research. Pragmatically, whilst the biggest medical challenges related to uterus transpants have been largely overcome for cisgender women, the reality is that transgender women do have anatomical and endocrinological differences which increase the risk and complexity of an already very difficult procedure. Governing boards have a huge reluctance for their institution to become the first to facilitate the gestation and birth of a baby by a transgender woman. Whilst the legal, ethical and medical obstacles are often cited, I suspect that the real issue is a belief that the resulting publicity would be largely negative, and damaging to both the organisation's reputation and its future funding.
Overall, transwomen are now being strongly discouraged by the medical
profession from even hoping that pregnancy is a real prospect for them.
Several transgender wome have
simulated on social media a pseudo 40-week pregnancy,
e.g. Gabrielle Darone gained considerable attention. By documenting
the daily challenges of balancing professional responsibilities with the
physical demands of wearing high-fidelity pregnancy prosthetics, she aimed
to replicate the experience of an expectant mother. Meanwhile, huge advances in AI are
allowing transwomen to easily create and post fake photos and even videos
apparently showing them pregnant, during child birth and breast feeding.
Most genetically XX women have the primary sexual organs that allow them
to become pregnant and gestate a baby. No genetically XY women has
these, no matter how young they transitioned with even the best quality
medical treatment.
The stress of being infertile, unable to get pregnant, not able to have
babies negatively affects the mental health of tens, if not hundreds, of
thousands of transwomen around the world. A particular problem is
those who identfied as a girl even before puberty. For example, a
now 26-year-old transwoman in the USA with two adopted children was
reported by the
New York Times
as: "craving to become pregnant ... I want the morning sickness, the
backaches, the feet swelling. I want to feel the baby move. That is
something I’ve wanted for as long as I can remember."
Until 2000 the idea of a genetic male (XY) being pregnant with a baby
was still in the realm of science fiction and movie makers, but since
then huge advances in female fertility treatment have made it a
possibility for transsexual women who are prepared to undergo the
required supportive hormone treatment and surgery.
By 2000 two
potentially viable medical procedures were identified to help
cis-women without a functional uterus who were seeking to bear a baby
(an estimated 1 in 500 women) -
an ectopic pregnancy or a uterus transplant. Both procedures are discussed below, but only the later
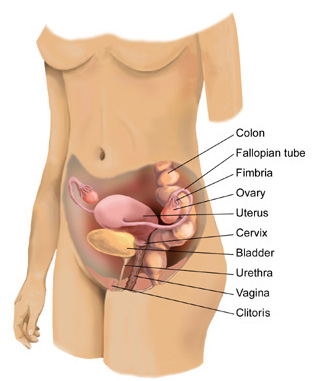
has so far emerged as practical. The Female Reproductive System Before going any
further it is necessary to consider the primary sexual organs needed to
become "pregnant".
Additionally, women have a unique secondary sexual characteristic
that for a million years was critical to the survival of a baby after
birth - their breasts can lactate milk.
When high-quality gender confirmation and
other feminisation surgery using modern
techniques is combined with hormone treatment,
the resulting external appearance - including the vulva - of many
young XY male-to-female (MTF) transwomen is indistinguishable from
that of a cis-woman at their peak fertile of age 20-30.
However, their neo-vagina does not lead on to a cervix.
Indeed, the cervix, uterus, ovaries, fimbria and fallopian tubes are
all missing. The reality is that a transwoman lacks the
internal organs required to become pregnant.
The internal anatomy of a XX woman (left) compared with a XY
transwoman after gender confirmation surgery.
Theoretically a dramatic hormonal and micro-surgery intervention on
an embryo with male XY genes might result in the development of a
baby with internal female sexual organs, but there is no obvious and
ethical reason for doing this.
Before 2000 an ectopic pregnancy - the development of
the baby outside the uterus (womb) - seemed the most likely procedure
for women without a uterus (including transwomen) as it was medically
simple because no transplants were required. The proposed technique involves attaching the foetus (the
term used for developing babies under 8 weeks from conception) to the
muscles inside the woman's abdomen, or an artificial womb formed from
abdominal tissue. Attachment to the bowel, with its good blood
supply, is another attractive option, but perhaps the worst in terms of
post-delivery trauma.
Unfortunatelym two big problems were identified with the ectopic
procedure: Natural occurrences of ectopic pregnancy do a occur,
however they are considered very dangerous to the mother. After 2000 interest in this procedure faded because of the
risks that it involves for the patient, and the advances that were being
made with uterus transplants.
Uterus Transplant
The possibility of uterus
transplants dates back to the origins sex-change surgery in the early
1930's. Lili Elbe (born Einar Wegener) famously had the one of the
earliest documented uterus implant operations in June 1931, age 48.
She sadly died just three months later from the complications.
After early failures, uterus
implants were not regarded as a viable approach. Experiments with
dogs and baboons in the 1980's were unsuccessful as it was found to be
very difficult to connect the required numerous blood vessels.
Pregnancy also puts huge strain on these connections, with very dangerous
consequences if something goes wrong.
However, in the 1990's
the concept of a short-term (one to two years) uterus implant purely to
bear a baby emerged.
Patients would still
need to take immunosuppressant drugs to help stop their body immediately
rejecting the uterus but researchers believed that the latest
immunosuppressant drugs did not have any negative effects on a foetus.
After the woman had her child, the transplanted womb could be removed,
avoiding
long-term risks
such as rejection
and undesirable side effects from the drugs.
This idea started what effectively became a competition for the first
successful pregnancy via a uterus transplant.
In order to reduce the high risks, it was desirable that the uterus came
from a woman with a close genetic match to the recipient, thus minimising
the chance of rejection. As the womb does not deteriorate greatly
from age it could come from a post-menopausal woman. According to Dr
Brännström "It could well be a relative. You could get it from your
mother. You could give birth to a baby from the uterus that you
yourself were birth from."
In January 2014, Dr Mats
Brannstrom revealed that the Gothenburg team had conducted nine womb
transplants on women who were born without a uterus or had it removed
because of cervical cancer. On 5 October 2014, one of these women -
Malin Stenberg - become the first in the world to have a baby after having
a womb transplant. The 36-year woman was born without a uterus,
received a donated womb from a "post-menopause 60-year old friend" in a
very long operation - it took a little over 10 hours to remove the uterus
from the donor, and just under five hours to stitch it into the recipient.
The
woman
must
take
immunosuppressive
medications
to
prevent
the body
from
rejecting
the
transplanted
uterus.
After
the baby
is born
and if
the
woman
does not
want
more
children,
the
transplanted
uterus
is
removed
with a
hysterectomy
procedure,
and the
woman no
longer
needs to
take
anti-rejection
medications.
For a transsexual woman absolutely determined to
start a family, a uterine transplant offers major advantages over
surrogacy. The transwoman is gestationally and socially clearly the
mother.
She can also control lifestyle factors such as smoking and drinking
alcohol, and she is the person who takes the health risks associated with
every pregnancy. But crucially, if the
foetus is created using her frozen sperm, then she is genetically as close
the baby as any cis-woman is of her baby.
On 15 February 2019 the Daily Mail newspaper quoted Christopher Inglefield, founder of the London Transgender Clinic, as saying "the procedure [for transgender women] is essentially identical to the one performed on women .. and it's important for trans females to be able to carry their own child." In February 2023 an article by Dr Flyckt and her colleagues at the Cleveland Clinic said that it was now a matter of when the surgery was conducted, not if: "The first uterus transplant in a transgender female [will] take place within the next few years, if not sooner. However not all doctors are quite so positive. Dr J. Richard Smith of Imperial College London, who co-led the first uterus transplant performed in the UK believes that “the transgender community have been given … false hope for responsible transplantation in the near future". He explained that even cisgender women who need surgery to create a neovagina aren’t eligible for the uterus transplants his team are offering as part of a clinical study. They have an altered vaginal microbiome that appears to increase the risk of miscarriage.
Ethical and Other ConsiderationsAn unusual aspect about uterus transplants is that currently they’re meant to be temporary. Typically, a woman receives a uterus via transplantation, its implanted with an embryo created via in vitro fertilisation (IVF), she gives birth via caesarean section and then has a hysterectomy to remove the uterus. This is very different from other more routine organ transplants like heart or liver transplants, which are intended to be permanent once they’re put into the recipient. A uterus transplant is also not a lifesaving procedure in the same way a heart transplant would be. There
are also questions concerning donation and the assignment of organs - for
example, what if a donor specifies that they only want to donate their
uterus to a cis-woman, and not to a transgender woman? There is then an
overlap with legal consideration as withholding a uterus to a transgender
woman could breach anti-discrimination laws. In the UK the
Human Fertilisation and Embryology Act 2008, states that an embryo
has to be implanted into a "woman", it would thus be illegal for an IVF
clinic in the UK to create an embryo for the purpose of implanting it in a
transwoman with a uterus transplant in order to make her pregnant. There
are also questions concerning donation and the assignment of organs - for
example, what if a donor specifies that they only want to donate their
uterus to a cis-woman, and not to a transgender woman? There is then an
overlap with legal consideration as withholding a uterus to a transgender
woman could breach anti-discrimination laws. In the UK the
Human Fertilisation and Embryology Act 2008, states that an embryo
has to be implanted into a "woman", it would thus be illegal for an IVF
clinic in the UK to create an embryo for the purpose of implanting it in a
transwoman with a uterus transplant in order to make her pregnant.However the later Equality Act 2010 supersedws this by clarifying that for legal purposes a transwoman is a woman, as long as they've gone through the legal process of being recognised as a woman. It would thus be illegal to refuse to a uterus transplant to a transgender woman solely because of they are transgender. Chloe Romanis, an Associate Professor in Biolaw at Durham University, Laura O’Donovan, a research associate at Lancaster University and Dr Hammond-Browning at Cardiff Law School, make several important points regarding transwomen having uterus implants which I have tried to aggregate these:
Dr Brännström believes that it might be possible to transplant a womb into transsexual women, allowing them to become pregnant with using donated eggs, though anatomical barriers would have to be overcome. "It should be technically possible, but I don't know if it's ethical."
The
crucial
caveat
is a
reference
to the
Montreal
Criteria
for the
Ethical
Feasibility
of
Uterine
Transplantation.
It's an
ethical
framework
published
in 2012
designed
to
assess
whether
a woman
could be
considered
as a
transplant
candidate.
Among
the list
of
qualifying
criteria
is the
requirement
that the
uterus
recipient
should
be a
"genetic
female
of
reproductive
age".
Whilst
surgeons
and
medical
teams
are
reluctant
to risk
not
complying
with a
widely
accepted
ethical
standard,
the
Montreal
Criteria
has
become
controversial
as it
prevents
transwomen
having a
uterus
transplant.
There
has thus
become a
campaign,
led by
Dr.
Jacques
Balayla
from the
McGill
University,
to
remove
the
reference
"genetic
female"
from the
Montreal
Criteria.
He
states
in an
interview
dated
March
2021
that: “A woman who is born without a
uterus and a man who transitions into a woman because of gender
dysphoria have a similar claim to maternity if we consider them to
have equivalent rights to fulfil the reproductive potential of their
gender. While still theoretical, it appears that implantation
of a donated uterus and gestation in the body of a transgender
individual should pose no physiological barrier if various
conditions are met." However, there seems to be no likelihood that the criteria will be amended
in the near future, so any surgeon or hospital conducting a uterus transplant on
a transwoman will be on a risky solo run. When the Montreal Criteria was
reviewed and updated in 2023, suggestions that the genetic female requirement be
removed were rejected. Assuming that the mother and her medical team have determined that the risks are acceptable, the key steps for a transwoman to become pregnant are:
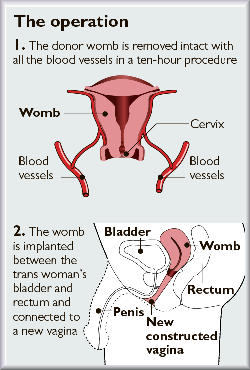
The diagram above shows the result of a theoretical uterus transplant procedure for a trans-woman. The transplant includes the cuff of the donors vagina, which is shown connected to a neo-vaginal canal probably constructed from penile skin and tissue - this is very useful for access to the uterus and clearing hormone induced menstrual flows. Obviously there are no ovaries and the uterine tubes have been truncated. After surgery there would be a c.12 week recovery period and the patient would require immunosuppressant drugs so that her body wouldn’t reject the new organ. The patient may need to wait a year before doctors will risk transplanting embryos into the new uterus, carefully prepared with hormones. If all goes well, the patient will become pregnant and carry her baby to term, for birth by C-section.
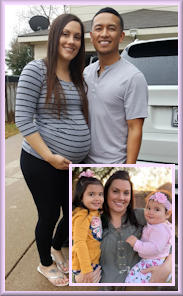
These images of Argentinean television celebrity Florencia de la Vega (Flor) provide a look into the near future. She was born Roberto Carlos Trinidad in 1995 and transitioned age 16. She thereafter worked as a showgirl and TV actress, and probably had SRS in 2010. In early 2011 she married Pablo Goycochea, age 36. Soon after, in August 2011, they announced the birth of twin babies - a boy and a girl. The story was presumably sold to the magazine Gente, whose front page showed Flor with the newborn twins whilst inside there was a carefully posed picture with her belly emphasised (or possibly wearing a fake silicone pregnancy belly) which could easily be mistaken for showing her pregnant with a baby bump. Whilst the supporting article repeatedly referred to Flor as the twins mother, it never explicitly states that she had been pregnant or had given birth to them. In fact the twins are the result of her husband's sperm being used to impregnate a surrogate mother, and she has no genetic relationship to them. The magazine then continued to regularly feature Flor and her children as they grew up.
A transwoman lacks the ovaries needed to produce an ovum containing her genes, and more specifically copies of her chromosomes. Thus, until the 2000's the primary method for a transwoman to gain a baby was having the egg of a surrogate mother being fertilised by sperm from her husband or partner, and the resulting baby being adopted after its birth. Clearly this approach is somewhat unsatisfactory for the transsexual woman as she has no genetic relationship with her baby.
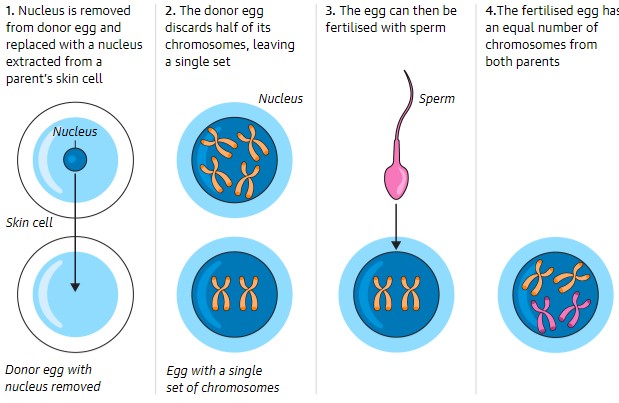
Also, for many years there has been speculation about potential new options which use a cloning technique called "membrane fusion" to create a fertilisable egg. A surprisingly simple technique has now emerged. Basically, a woman donates an ovum egg. The nucleus, containing this woman's DNA, is removed, and a nucleus with genes extracted from one of the transwoman's skin cells is put into its place. The ovum realises that this has too many chromosomes and discards the half of them, thus creating an unfertilised egg with just one set of 23 chromosomes. Using standard IVF techniques the new ovum can then be fertilised by the father's sperm and implanted into the uterus of a surrogate mother. Both the mother and her husband/partner will have a a normal 50% share of the baby's gene's.
When the first version of this page was drafted in 2001, the idea of a genetically XY male-to-female transsexual becoming pregnant was still close to science fiction. Over 20 years later it's clear that all the major medical barriers have now been overcome. Indeed, it is quite possible that somewhere in the world (most probably in Brazil) a transwoman has already quietly given birth.
The next problem is cost. Uterus transplants are only just moving from research to mainstream, and as such are still being hugely subsidised. Although uterus transplants are starting to become an accepted medical procedure, few public health services or health insurance policies are likely to cover them due to the very high cost, indeed health insurance policies are starting to specifically exclude it. The UK's NHS estimated in 2020 that prospective "routine" uterus transplants procedures involving a cis-woman would cost about £50,000, however this was just for the two operations (donor and recipient) plus immediate pre- and post-operative care. Other estimates are even higher, in 2019 the American based UTX group estimated $200,000 for a uterus transplant, whilst an article in PubMed estimated €50,000 to €100,000 (mean €74,000) in Year 2020 values per uterus transplantation. The total medical costs over 3+ years for a transgender woman to go through all stages from gender confirmation surgery, uterus transplant, pregnancy, birth and finally uterus removal could easily be £/€/$ 1 million. And that is just the direct medical expenses, without even including other factors such as loss of earnings. Pregnancy and motherhood seem likely for many years to be a privilege reserved for transwomen with substantial personal wealth or a rich husband.
Part 2 of "Transsexual Pregnancy"
(c) 2000 - 2026 Annie Richards Please send any comments, feedback or additions to: Last updated: 8 January, 2026
| |
 When
I published the first version of this page in July 2001, I was certain
that within twenty years transgender woman would be routinely getting
pregnant and delivering a live baby as its mother. Sadly I was
wrong.
When
I published the first version of this page in July 2001, I was certain
that within twenty years transgender woman would be routinely getting
pregnant and delivering a live baby as its mother. Sadly I was
wrong. 





 The
internal reproductive organs of a genetically XX woman include:
The
internal reproductive organs of a genetically XX woman include: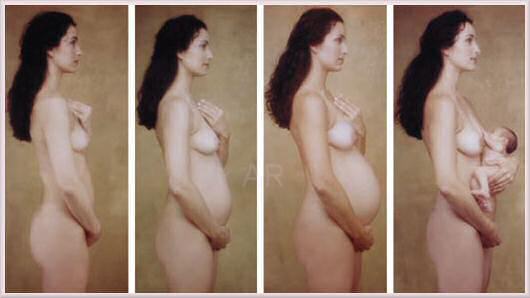




 A
A Researchers
then sought better ways of "plumbing in" the transplanted uterus than the
Saudi's had used. In
June 2003 a Swedish team led by Dr Brännström of Sahlgrenska University
in Gothenburg, announced a new technique where the transplanted womb is
attached to two arteries and three veins on each side, with blood
primarily coming from the external iliac artery. It would also be
attached to the vagina, and to the round and sacral ligaments to hold it
in place, but not to the Fallopian tubes - if the woman has those.
The woman would not be able to conceive naturally, but would have to have
IVF. She would also have to give birth by Caesarean. The
technique was considered simpler and less risky than most transplant
operations
Researchers
then sought better ways of "plumbing in" the transplanted uterus than the
Saudi's had used. In
June 2003 a Swedish team led by Dr Brännström of Sahlgrenska University
in Gothenburg, announced a new technique where the transplanted womb is
attached to two arteries and three veins on each side, with blood
primarily coming from the external iliac artery. It would also be
attached to the vagina, and to the round and sacral ligaments to hold it
in place, but not to the Fallopian tubes - if the woman has those.
The woman would not be able to conceive naturally, but would have to have
IVF. She would also have to give birth by Caesarean. The
technique was considered simpler and less risky than most transplant
operations












 Back to Articles
Back to Articles