
Important Disclaimer: The information on this page is often historical and should not be used to guide surgical decisions.
The first version of this article was written in 1999. At that time, the term "transsexual woman" commonly meant a man who had, or was planning to have "sex re-assignment surgery" (SRS). This article still often uses the abbreviation 'SRS' rather than more recent and possibly more accurate terms such as Gender Reassignment Surgery (GRS) or Gender Confirmation Surgery. The term 'Bottom surgery' has also become a common term since 2015. Some Background
A huge change in the last few decades - at least in the "west" has been the reduction in the age of the patient having GCS. In the UK the average medium age for GCS performed by the NHS on a transwoman was 42 in 2000, it had decreased to 36 by 2016, and was just 23 in 2023!
Sex re-assignment surgery arguably goes back thousands of years - particularly if castration is accepted. In the 4th century BC Aristotle was accurately describing the physical results of male castration, and attractive young eunuchs were often the preferred sexual partner(s) of Kings and Nobles in Asia, Africa and beyond.
In ancient Rome, slave owners often ordered the castration of boys whom
they sexually enjoyed in order to prevent a male puberty. The
castrated boy
was known as a puer delicatus or deliciae (meaning
sweet, dainty). One such such castrated boy
would even become the Empress of Rome - twice!
A few
Chinese eunuchs were castrated before puberty - typically by age ten.
These were
considered ‘thoroughly pure’ because they had never experienced sexual
desires. Unlike older eunuchs, after castration they usually dressed
and lived as a woman. Due to their feminine appearance and speech they were prized as personal servants and
concubines. Some were considered
so beautiful that they became the acknowledged
'companion' or even the official wife of a senior official - the later including
other important eunuchs!
In the 21st century, castration - aka bilaterial
orchidectomy -
has become a common voluntary procedure among transgender women.
It is a very cheap and low risk procedure that prevents further
masculinisation from testosterone hormones, whilst aiding feminisation
from taking oestrogen.
Surgery Becomes An Option Christine Jorgenson's surgeries in Denmark and the USA between 1951 and 1953
are widely accepted to be first attempt using modern surgical
techniques to create female genitalia from male genitalia -
including a vagina. The Harry Benjamin
International Gender Dysphoria Association periodically publishes
standards of care for hormonal and surgical reassignment, and most
medical professionals follow this. I.e. reputable surgeons will
refuse to perform SRS on a patient who does not fully meet the
standards. The key points of the 2001
version of the standards are: SRS
involves major surgical procedures by which the physical appearance and function of
male genitalia are altered to resemble those of a female.
The
ideal results are: However, like all
major surgical procedures, SRS is expensive, very painful, has many
risks and there can be serious complications. There are many transwomen who
take oestrogen hormones and live, work and socialise as a woman, but never have SRS. The first recognised SRS
procedure only occurred in 1952, but numbers have grown rapidly ever
since - from dozens annually (world-wide) in the 1960's to tens of
thousands a year by the 2010's. About 800-1000 MtF SRS operations were
currently being
performed in the USA each year, and that many or more were performed
on American citizens abroad The top three USA surgeons (Eugene Schrang,
Toby Meltzer and Stanley Biber) together performed a total of 400 to
500 SRS operations each year. Adding together the raw numbers
suggested 30,000 to 40,000 post-SRS women in the USA, however some must
have died since having SRS. Given that most operations
been performed within the past 15 years, it was reasonable to assume that
a high percentage of thesewere still living. Also, she found that
transwomen who underwent SRS in the 60's to mid-80's were often young - in
their twenties and early thirties, and thus most of those women were also
still alive. So, even
accounting for mortalities, Lynn estimated that the total number of
post-SRS women in the US was greater than 32,000 at the end of 2002. In the UK, a BBC report in 2007 claimed that there were 15,000 post-SRS
transsexuals in the United Kingdom but this seemed improbably high.
Perhaps more
accurately a
Gender Variance report in 2009 estimated that in the UK there were
10,000 transitioned transsexuals, 3,500 of whom had had SRS - of which 80% of
were MTF, implying 2,800 post-operative transwomen. Since
the mid-2000's numbers have been increasing dramatically. In the United
Kingdom, the National Health Service (NHS) performed 137 SRS operations (all MTF) in 2009
(compared to just 54 in 2004); another 90 were funded by UK health
insurance companies; and the Gender Identity Research and
Education Society charity estimates
that at least 150
such procedures are paid for personally by the patient each year - these are usually performed overseas,
most commonly in Thailand or the USA. I.e. a total of perhaps 380
UK residents had male-to-female surgery in 2009. In the UK, in 2013 the NHS received 2,500 new referrals of
patients with gender dysphoria, just two years later this was nearly 4,000 (a fifth of which were under age 18).
Historically about half of the referrals will eventually has SRS. The NHS currently has the capacity to perform about 480 MTF
SRS procedures a year, but 1,800 patients are expected to be added to the
waiting list in 2016. To avoid years of waiting, many
British transwomen choose to pay to go private, mostly to surgeons in Thailand and the USA. Based on trends,
a reasonable guesstimate is that about 1,000 UK residents had
male-to-female sex re-assignment surgery in 2015 (compared to 9,000 in
the USA). This leads to
the projection that there were around 16,000 post-SRS women
in the country in 2020 (about
1 in 2000 of the female population). Of these (allowing for deaths),
less than 1000 had their SRS before 2000! It should also be noted that whilst SRS patients in their teens and twenties have
been commonplace in
Asia and South America since the 1980's, it was rare in Europe and
the USA before the 2010's. The UK is just a very small element of a global picture,
with "sex change hospitals" around the world each now performing
hundreds if not thousands of procedures a year. Whilst clinics in
Thailand have the most publicity
(e.g. Chettawut Plastic Surgery Centre, Sava Perovic Foundation Surgery,
and Phuket International Aesthetic Centre), there are also lower profile
but still very substantial clinics in the USA (e.g. Rumercosmetics, Transgender Surgery Institute of Southern California,
Mount Sinai Centre for Transgender Medicine and Surgery) and in other
countries such as Germany, Australia and Brazil. I've attempted and failed to find good statistics on the number of MTF
SRS procedures
that have been performed, but a cumulative total of one million at some
point between 2016 and 2020 seems certain. If forecasts of a
continuing 25% annual growth are correct then the number could easily
pass two
million by the mid-2020's
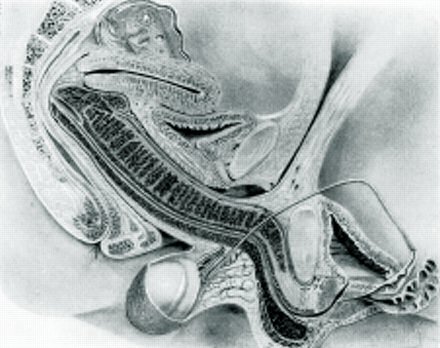
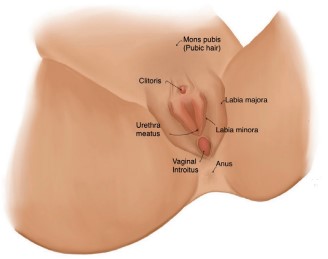
The diagram to the right compares the organs of a male and
a female
in abdomen region. The immediate standout is the primary sexual
organs of the male - the prominent penis and testes. The removal
of these makes the two diagrams much more similar - and it's much easier
to surgically remove tissue than add! It takes a closer
examination to reveal the woman's primary sexual organs - her ovaries
and uterus. However, there is currently no way that these can be
replicated except by very risky and costly implants. A final examination
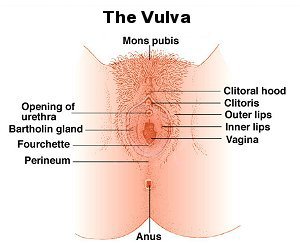
of the diagrams alights on the path of the female urethra, the vagina, and the extraordinarily complicated vulva area
of a woman.
Counting Christine Jorgensen's penectomy operation
in 1952 as the first real SRS, surgeons have essentially spent 65+ years
refining their procedures for these.
Most
surgeons will consider as eligible for SRS genital surgery a
genetically male "woman" over the age of majority who has
undergone at least 12 months continuous female hormonal
treatment, and who's also successfully lived for at least a year
full-time as a woman. However, a surprising large number
of women who fulfil these criteria do not immediately seek SRS,
or any other genital surgery. The reasons for delaying or
avoiding SRS procedures are very diverse, but include:
Unfortunately, I haven't yet found any recent (rather than 1960's)
statistics on the length of time after a real-life transition until
genital surgery for male-to-female- women, but I have found some
interesting figures for female-to-males.
. These
extraordinary results are not directly relatable to transsexual women as
much more difficult and expensive surgical procedures are required for
female-to-male sex re-assignment than for male-to-female sex
re-assignment. However they do reinforce my own belief that a
medium [average] delay of 3 years from full time transition to MTF SRS
would probably be near the mark, high though this may appear at first
sight given that a common complaint from transsexual women is the need
to wait a whole year after transition before being eligible for surgery. But the
reasons to have some form of genital surgery often strengthens with
time, and most transitioned transsexual women eventually undergo
some procedure. Possible drivers may include: The importance of the
second point cannot be underestimated. Most post-transition but
pre-SRS women gradually collect bad experiences, ranging from
embarrassment during a security check, an unaware friend who sees too
much, the wandering hands of a drunk, to the possibly fatal
disappointment of a rapist. In a few countries, a
depressing problem is that some homosexual men have sex-change surgery
because it is socially and legally more acceptable to be a transsexual
woman than an openly homosexual man. Iran is most commonly cited.
(Note: this must not be confused with the
homosexual transsexual theory).
No
surgery. Prolonged
female hormonal treatment will shrink
the male genitalia significantly and will eventually cause permanent
chemical castration after about 6-12 months use.
Surgical Castration or
Bilateral Orchidectomy. The removal of the testes (or
gonads) along with the undesirable masculinising and
virilizing effects caused by the testosterone that they produce.
Limited SRS - vulvoplasty. This involves
the removal of the testes and penis and the formation of
female appearing external genitalia, but with no emphasis on
vaginal depth. A labiaplasty will often follow to improve the vulva's
external appearance.
Full SRS- vulvoplasty and vaginoplasty. Removal of the
testes and penis and formation of female appearing external
genitalia, plus the creation of a neo-vagina with adequate
depth for intercourse.
A labiaplasty will again often follow to improve the vulva's
appearance.
The decision on which
option to select is a personal choice that may well evolve over time.
For example, most men who believe that they are transsexual will start
off assuming that they will have SRS as soon as possible when they seek
treatment. However, after they have benefited from hormones (etc.)
and perhaps transitioned to live as a woman they may no longer see any
urgent need for SRS and it’s only some event years later such as a
relationship with a heterosexual man that eventually causes them to have
SRS.
If
there are any doubts, the best route is always NO surgery. It’s
always possible to have surgery later, but it’s impossible to
reverse castration or SRS. Even if surgery is decided on,
the prior freezing of a sperm sample (if obtainable) may be a
sensible measure to help preserve some reproductive options -
even as a mother.
For SRS
a variety of techniques are used. By far the most common
is variations of the Penile Inversion method. A less
common procedure is variations of the Sigmoid Colon Section method,
or Colovaginoplasty.
Other techniques include the Scrotal Inversion Procedure and the
new Peritoneal Pull-Through Vaginoplasty Procedure. SRS always involves the formation of the entrance to
neo-vagina (i.e. an artificial vagina). However for various
reasons this can be often be quite shallow (just 2-3 inches, 5-7cm).
The decision as whether to have a deep vagina suitable for penetrative
intercourse by a penis need not always be an automatic "yes" -
particularly for elder women who perhaps don't intend to lead an active
sex life after surgery. Reaching and then maintaining full vaginal
depth often requires the effort of regular dilation and/or then frequent
sexual intercourse. An
interesting debate about the merits of two most popular SRS procedures
can be found
in the link
here, but the accepted pros and cons are summarised in the table
below: Patients who expect to have very active sex life as a woman often
opt for the colon procedure. However, the
penile inversion procedure (or minor variants of this) remains the
dominant procedure recommended by surgeons. Whilst it's still major
surgery, the risk of serious complications is much lower (perhaps just 1%) and the procedure has been refined to reduce earlier
problems such as vaginal hair growth. The need for time consuming
dilation in order to maintain vaginal depth has become the biggest
complaint from patients. The following factors will influence the results of the SRS and
the depth of the vagina: It is important to re-iterate that the prolonged use of
hormones and an orchidectomy has a very negative effect in
relation to SRS as in time the penis and scrotum will atrophy to
some extent, i.e. the penis size reduces and the scrotal sack
shrinks. The earlier that SRS is performed (ideally before
hormones are even started!), the better the likely result,
indeed some leading surgeons who are anxious to preserve their
reputation are reluctant to perform surgery on a patient who has
previously had an orchiectomy. Of course this situation
contradicts the recommendation of many psychiatrists that a
lengthy "real life test", usually associated with a hormone
regimen, is essential prior to any genital surgery.
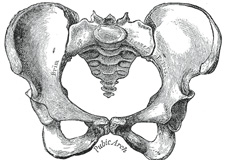
In general genetic women (regardless of their height)
have broad hips, i.e. a broad
pelvis with a pelvic cavity offering plenty
of internal volume. They also have a wide pubic arch and a large
oval-shaped pelvic inlet – ideal both for giving birth and for sexual
intercourse. The result of this skeleton
is that even an otherwise petite woman can comfortably and enjoyably
accommodate a large penis. Unfortunately arrangements don’t tend
to be quite so satisfactory for transwomen - in general they have a
narrow pelvis, a tightly angled pubic arch, and a small, partially
obstructed, heart-shaped pelvic inlet. For the majority of
transwomen their skeletal structure would theoretically rule out natural
delivery of a baby, and rather more relevantly the pelvic bone
structures of a minority may unnaturally (for the man) impede or even
obstruct a penetrating penis, and also restrict the degree and direction
that a neovagina can stretch to accommodate the penis.
Another issue is that fact that genetic woman have a strong muscular and
ligament framework surrounding their vagina - muscles which act upon the
penis during intercourse whether controlled consciously or
unconsciously. Transwomen do not have any true vaginal muscles
after their SRS – however a combination of frequent internal exercising
and an active sex life can result in very satisfied male partners.
With modern techniques, surgery at a good clinic is likely to result in a single operation in an external physical 'bottom' appearance
that is sufficient (particularly with pubic hair) to not to have to worry
in female changing rooms or having sex in a darkened room.
Post surgery
problems tend to relate to scaring, a high
vulva/vaginal position (due to skeletal limitations) and an excessively
large clitoris. Admittedly, achieving a visual appearance that
on intimate examination in daylight is hard to distinguish from a natal women
is still likely to require revision
surgery to tidy things up, e.g. the labia and clitoral hood. For successful intercourse, arguably
sensitivity and even appearance (it's 3:00 am, dark, and many pints and a
bottle of vodka have been consumed ...) are less important than the fact that the neovagina feels totally natural to the man, particularly if the woman is
stealth. Adequate depth is just one factor, others include
adequate lubrication and the woman’s internal anatomy.
Some transwomen place great emphasis on having a natural looking
vulva area, for example a transwoman working as a female model will
frequently have to pass nude backstage with numerous strangers. Other
transwomen may prioritise a sensitive clitoris over good vaginal depth, for
sexual reasons that include lesbianism and masturbation desires. Overall, it is highly recommended that a transwoman
planning to have SRS carefully research both the best procedure
and the best surgeon that is likely to best meet her priorities - albeit
with no absolute guarantee of success.
Penile inversion vaginoplasty procedure:
The penile inversion technique was pioneered by Dr Georges
Burou who first used it at his famous Morocco clinic in 1956. Its
original success was due to its sheer simplicity, albeit still
involving major and risky surgery. Critically it gave patients
a functional vagina, often indistinguishable by men from that of a
cis-woman. Whilst the external appearance of the vulva
in procedures up to the 1970's often amounted to no more than a
slit-like entrance to the neo-vagina, the growth of pubic hair and
restricting intimacy to a darkened room often avoided any problems.
The procedure has
since been greatly refined and improved, and as of the early 2000's it remains by far the most
commonplace MTF SRS procedure - if only because its advantages and
problems are so well known by both surgeons and patients.
The penile inversion technique generally produces satisfactory
aesthetic and functional results, although these may of course vary
depending on the age, weight, quality and elasticity of the skin,
and the overall health of the patient. A typical result
by an average surgeon is:
Six to twelve months after SRS the swelling will have gone, tissue
will have healed, scares faded and pubic hair grown. The genitalia
of the woman are then very likely to be passable when nude in a changing
room context, and possibly even in an intimate relationship.
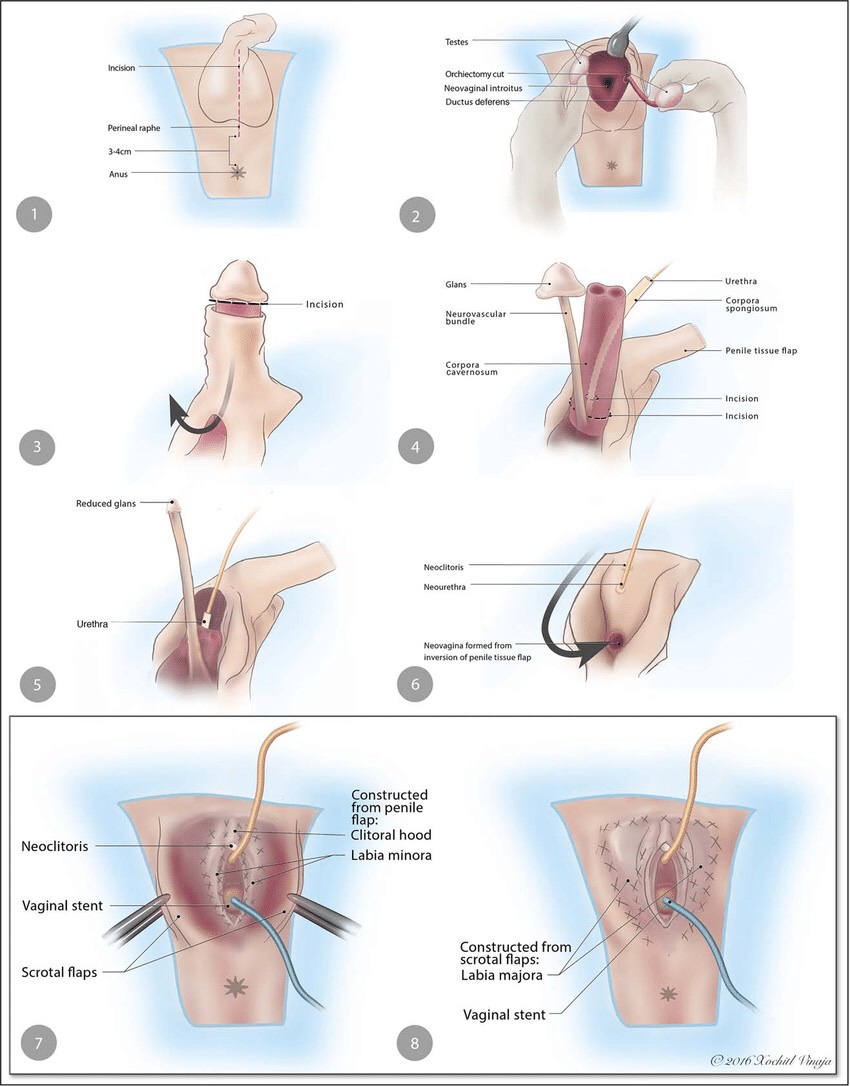
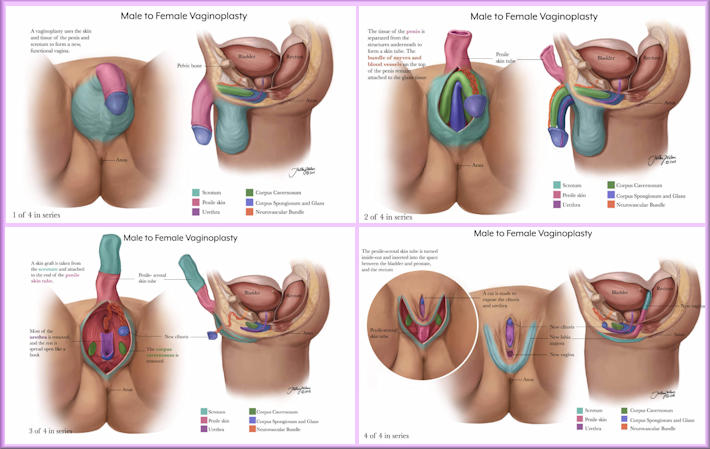
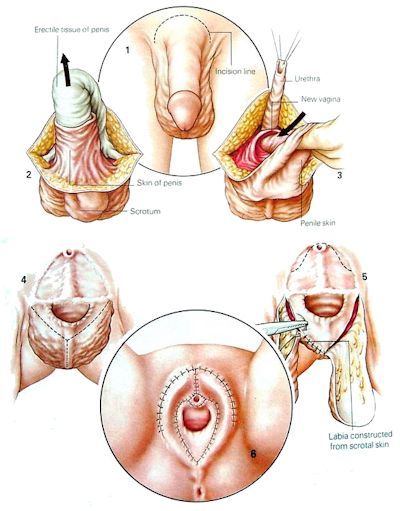
An Overview of Male-to-Female Sex Reassignment Surgery
(Vaginoplasty) 1) An incision is made on the scrotum and the testicles removed.
Most of the penis is amputated, but the skin and nerves are
carefully preserved.
Another
representation of the "penis inversion" Male-to-Female Sex Change
Procedure
1.
An incision is made around the base of the penis. A major disadvantage
of the penile inversion procedure is the limited depth of the
neo-vagina. Most patients will have been taking female hormones
for the several years and as result their penis will have greatly
shrunken in size. For satisfactory
penetrative sexual intercourse with the averagely endowed man, a
vaginal depth of 6 inches (15 cm) is required. Unfortunately,
this is difficult to achieve with the popular penile inversion SRS
procedure -
using just
penile skin may result in a vaginal depth as shallow as 2 inches (5
cm). After a year of diligent dilation, the likely depth is still just
4 - 5 inches (10 - 12.7 cm). Insufficient vaginal depth is the
biggest single cause of dissatisfaction in the results of SRS using
the penile inversion technique.
To accommodate the
penis of a well-endowed male partner, a vaginal depth of up to 9”
(20-22cm) is necessary. Whilst many natal cis women will also
have a problem fully accepting such a lucky man, their vagina is very
stretchy in nature and doesn't have the dead-end of a transwoman's neo-vagina. The best surgical options for a
very deep neovagina are a colon graft or peritoneum flaps - but even
then the transwoman's pelvic skeleton and internal organs may limit during
sexual intercourse the mimicking of the vagina of a genetically XX
woman with an exceptionally well endowed man. For example (as noted above), the narrow pelvic opening of
most transwoman will physically prevent their neovagina accommodating a
penis with a girth much greater than 5"(13 cm).
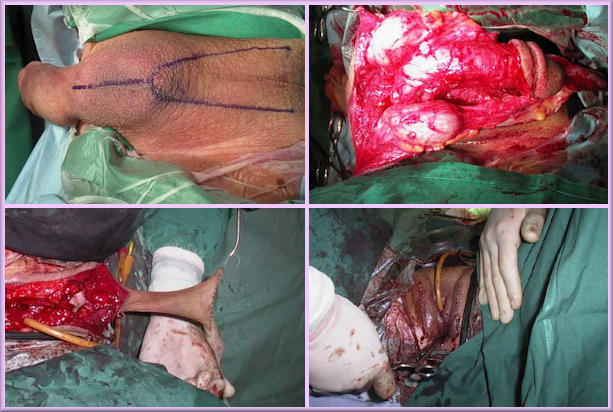
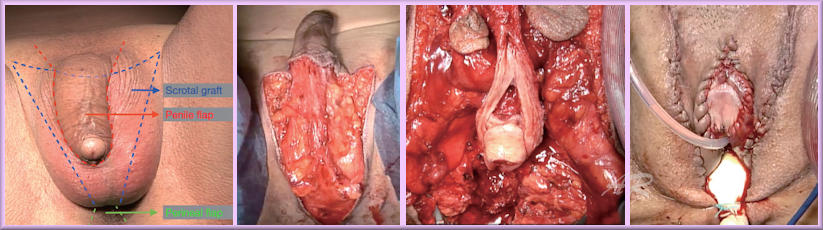
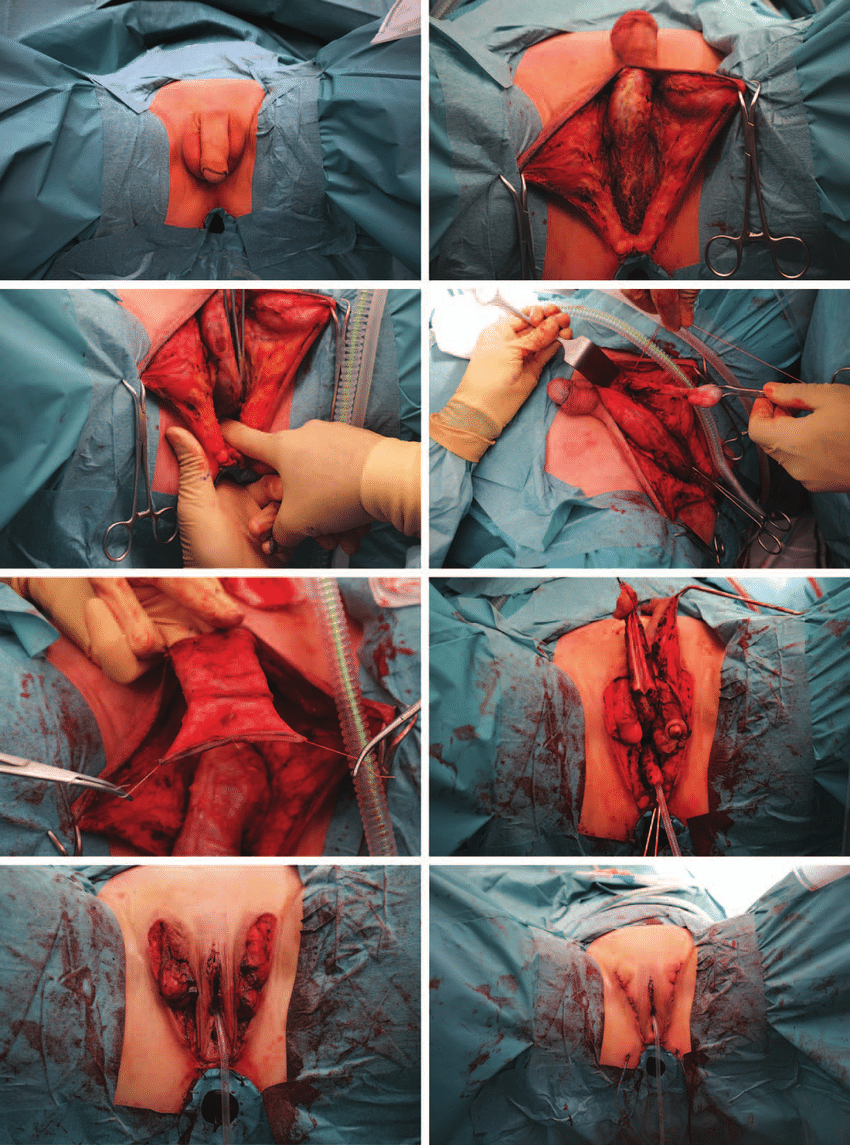
A picture sequence of a 53-year old transwoman have
SRS using the penile inversion technique:
Click on the picture below for a photo gallery of a patient undergoing
sex re-assignment surgery using a variant of the penile inversion
technique, with a scrotal skin graft to increase the depth of her neovagina.
The procedure begins with an incision down the centerline of the scrotum
from the base of the penis and a catheter is inserted into the urethra.
The muscles making up the pelvic floor are separated to make a path for
the neovagina to pass through and into the body. The ductus deferens are
cut and the testes removed (and sent to pathology for examination). Then
a radial incision is made on the skin of the penis just under the glans
and the penis skin is dissected from the shaft.
The degloved penis is
pulled through the skin into the scrotal opening and is further
dissected: the corpora cavernosa are separated and cut off at the base
and discarded; the urethra and the glans cap connected to the
neurovascular bundle are retained.
The glans is reduced by removing
epithelial tissue — this becomes the neoclitoris and is placed at the
base of the corpora cavernosa via a small incision in the skin which had
been at the top of the base of the penis.
Another small incision is made
about 1 cm below there and the urethra is passed through and cut at skin
level and both are sutured into place.
The penile shaft skin is sutured
together at the glans end (sometimes additional skin is attached to give
extra depth, then pulled inside out such that the epidermis is on the
interior of the resulting tube. This is fed between the pelvic floor
muscles and form the neovagina. A stent or packing is inserted to hold
the shape of the neovagina for the first week.
Skin from the base of the
penis is reformed to make labia minora, and scrotal skin used to make
labia majora, which closes the body back up. Sometimes excess scrotal
skin is used to add depth to the neovagina before the skin is inverted
and inserted.
Non-Penile Inversion Procedures
In
Western Europe and North America penile inversion vaginoplasty
remains by far the most common SRS technique. But there are alternatives.
The sigmoid colon section vaginoplasty procedure is the next most popular SRS technique after penile inversion. This uses a section of the sigmoid colon to create the vaginal lining.
It is an intrusive procedure in which the
intra-abdominal cavity must be entered via a low transverse abdominal
incision (similar to a caesarean section incision in a biological female).
A sigmoid colon section approximately 6-7 inches in
length is cut out and harvested
through the incision, with the rest of the colon reconnected. This
extracted segment of the lower colon is thick-walled, large in
diameter and flexible. The colon section is then relocated and connected to external genital skin flaps to construct
a neovagina and its entrance. Orchiectomy, penectomy, labiaplasty and clitoroplasty
procedures are performed as required to create the external appearance
of a female vulva.
The procedure is also very suitable for patients who have a have a very small penis, e.g., due to an orchiectomy. It is can also be used as corrective surgery for patients with inadequate vaginal depth after penile inversion SRS. However, although the procedure is well proven, both the cost and medical risks are higher than the penile inversion procedure because of its more complex and intrusive nature.
In Thailand - where nearly as many SRS procedures are performed annually as the rest of the world put together - most surgeons use a scrotal inversion procedure. Instead of the penis, they use the scrotum to create a vagina. A major advantage is that the scrotal skin can be stretched, so a small penis is less likely to affect vaginal depth unless an orchidectomy (castration) has already been performed. During the surgery the surgeon will remove the hair follicles from the scrotal skin, so electrolysis is not required - but subsequent hair growth their vagina is reported by some patients. The surgeon will try not to remove the bulbourethral glands (Cowper's gland's) as these help to provide lubrication during sexual arousal. Immediately after surgery, 15 cm (6 inches) of vaginal depth is typical, and 18-19 cm (7 inches) common. Post-surgery dilation is still required to maintain depth, but it's slightly less demanding than penile inversion where the dilation is often trying to increase vaginal depth. Although the penile inversion procedure is clearly considered in medical publications to be a superior and and more advanced procedure, there is no doubt that Thai surgeons are consistently achieving excellent results with this technique.
Penile Peritoneal Vaginoplasty (PPV) The peritoneal pull through procedure was originally developed in India in the 1960's as the 'Davydov technique', to help natal cis women who were born without a vagina. The peritoneum is basically a bag of loose tissue that encircles the inside of the abdomen and holds the guts in place, and it is very similar in characteristics to the lining of a vagina. It surprisingly took nearly 60 years before it was realised that a variant of this procedure could be applied to sex-reassignment surgery. This procedure uses a small amount of penile inversion combined with a peritoneum pull through technique to create the neovaginal canal. Essentially the outer labia and visible vagina is made using penile and scrotal skin whilst the inner vaginal canal is made using the peritoneal.
During surgery, a laparoscope and several instruments are inserted through small 5-8 mm incisions on the abdomen. These instruments are used to create a space between the lower urinary tract (urethra, prostatic urethra, and bladder) and rectum. This space will become the future vagina. Abdominal (peritoneal) lining is then pulled through to the area between the urethra and the rectum to line a portion of the vaginal canal. The top of the new vagina is separated from the abdominal contents by closing the peritoneal lining approximately 15 cm from the vaginal opening. The remainder of the vaginoplasty procedures (labiaplasty, clitoroplasty, penectomy, orchiectomy, partial urethrectomy, and other associated procedures) are similar to that of the penile inversion technique.
Claimed advantages over other techniques include a quicker and painful recovery, far less visible scaring, and less dilation and douching. Perhaps the decisive factor for many transwomen is that the resulting neo-vagina is apparently often indistinguishable by a man from that of a cis-woman when having intercourse. The lubrication, elasticity, depth and smell are also supposedly excellent. Restrictions and discomfort related to the shape of the transwoman's pelvic girdle are the most likely problem if the man is well endowed. Despite the apparent positives, it is important to realise that this is still a very new procedure and that the surgeons who are using this technique are inexperienced with it. The initial excitement will dissipate as problems and risks inevitably emerge. I have struggled to find patient feedback and where I have it is often far from positive, indicating that the procedure is not a panacea and that serious complications can occur. For example, the promise of a neo-vagina with good depth that doesn't require dilation is not confirmed by some patients.
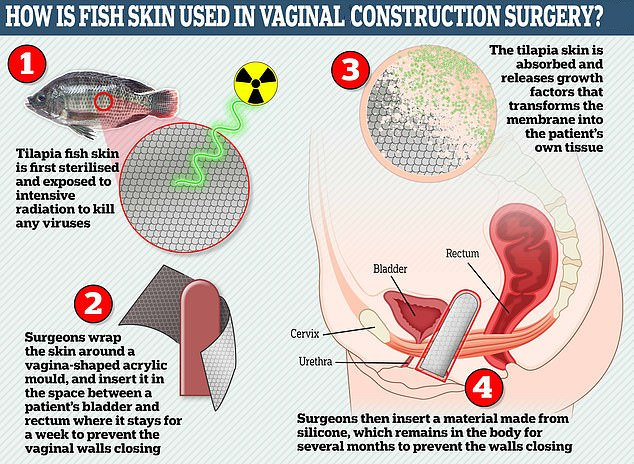
A recently developed technique to help the development of a neovagina is the use of tilapia fish skin! The first procedure on a transwoman was only in April 2019, but it has rapidly gained in popularity. In this procedure a vaginal acrylic mould covered with processed and sterilized tilapia fish skin is inserted and accommodated into the newly created cavity. The grey external side of the tilapia skin (scales removed) stays in contact with the acrylic mould, while the white internal side of the tilapia skin, which was previously attached to the fish's muscle, is in contact with the walls of the neocavity. The mould is held in position by sutures in the labia majora, thus preventing expulsion.
The patient remains in bed rest for 9 days, by which time the tilapia fish skin has been partially reabsorbed and has encouraged the development of vaginal wall tissue. The acrylic mould is removed and a larger plastic mould (8-9 cm long) is inserted, the patient is advised to wear this day and night for a month. She then needs to wear it every night unless engaging in regular normal sexual intercourse. Analysis of the neovaginal wall of one patient 180 days after surgery showed the presence of a stratified squamous epithelium with five cell layers, small ectatic (swollen) blood vessels and occasional desquamated epithelial (shedding) cells - not perfect but significantly better than the neovaginal lining of most transwomen.
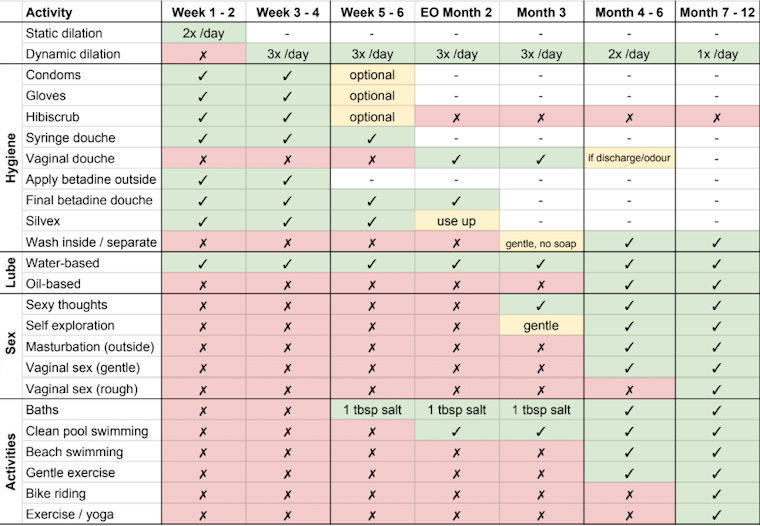
Maintenance of a Neo-Vagina Vaginoplasty involving the creation of a vaginal cavity requires on-going care that the woman will have to integrate into her daily routine for the rest of her life. This care involves a protocol of regular vaginal dilations and genital hygiene. Failure to follow the recommended procedures could result in the closure of the vaginal cavity; difficulty in urinating; as well as complications such as urinary tract and other infections, sores and vaginal discharges, and abnormal communication between the vaginal and rectal cavities . Whilst the exact regimen is dependent on the procedure that was used, the transwoman will need to:
Pelvic floor exercises developed primarily for women after childbirth are theoretically irrelevant for transwomen, but in practice many transwomen have found them to be very helpful. The exercises can mitigate painful or insufficient vaginal dilations, as well help any urinary leakage after surgery.
Vagina Not Required Zero-depth vaginoplasty includes rearranging the tissues of the penis and scrotum to generate a vulva (sensate clitoris, clitoral hood, labia majora, labia minora) and a functioning urethra. The visual apprearance is that of a woman, but a vaginal canal is not be created. This treatment allows for a functional outward look that corresponds to a person’s gender identification. The 'penis/dildo penetration not required' approach offers the transwoman significant health and hygiene benefits, possibly too many surgeons and patients focus excessively on the creation of a deep neo-vagina which may not be necessary - particulay for older patients. The emphasis can instead be place on achieving the best possible external appearance, rather than on sexual functionality and enjoyment. For example, surgeons find it difficult to construct from a penis a sensitive clitoris of natal female size and thus often have to balance sensitivity with avoiding excessive size - this conundrum disappears if 'good sex' as a woman is not a driver for SRS.
Note:
Since writing
this section, one transwoman has contacted me expressing
Age at SRS For decades after Swede Christine Jorgenson had her pioneering SRS in 1957, most empirical evidence and published studies have indicated that a majority of European and North American transsexual women are in their 30's, and 40's before they actively seek to resolve their gender issues. Inevitably this means that the patient age profile of surgeons undertaking sex-re-assignment surgery follows this trend - with a lag of a several years representing the time from the woman commencing treatment to having some form of genital surgery.
Considerable publicity often surrounds young transsexuals who with the support of their parent's transition have surgery at a very young age - in their teens or in exceptional cases even earlier. There is no doubt that this group is rapidly becoming more numerous, but it is still only a small proportion of the transsexual community. There is also a statistically significant group of young transsexual women (often from parts of Asia and Latin America) whose career in the sex industry leads to various surgery procedures in during their teens and 20's, but this is usually in the form of breast augmentation and facial feminisation. When (or if) they finally decide to have SRS, typically in their 30's, it generally marks their move out of the sex industry,
The following table shows the
age of MTF transsexual women receiving SRS between 1997-2000 at one
clinic in Thailand:
Nationality
Average age
Lowest age
Highest age
Total number
One rarely mentioned problem that a transwoman faces after SRS is that her new vagina lacks the complex community of 'good' micro-organisms that help to keep the vagina of a natal cis-woman healthy. In cisgender women, i.e., those assigned as female at birth, an optimal vaginal microbiota includes microbial communities such as the Lactobacillus species. These microbes play an important role in preventing unpleasant bacterial infections (including sexually transmitted and urinary tract infections), vaginal discharges, and an excessively strong fishy smell emitting from the vulva area. They also reduce or eliminate the need for douches or vaginal washes. Unfortunately for MTF transgender women, the pH in penile inversion (i.e. skin-lined) neovaginas is elevated after surgery, discouraging the growth of acidic preferring Lactobacilli, with colonisation of bacteria from skin or intestinal micro-organisms occurring instead. Their neo-vagina is thus very likely to inherit the bacteria that populate penile skin such as Porphyromonas - these are less helpful and may increase susceptibility to recurrent neovaginal infections. A possible solution being explored in 2019 by John Hopkins University in the USA is the use of vaginal fluid transplants. The concept is very simple - a donor woman inserts and then removes a flexible plastic disc - similar to a menstrual cup or a contraceptive diaphragm - to collect fluid from her vagina which is filled with 'good' bacterium. The fluid is then drawn up into an applicator for the MTF recipient to insert into her neovagina a similar way to a tampon. Hopefully the newly introduced bacterium will then populate and multiply in their new home and reduce undesirable infections and their side effects. If the trial results are good, this may become a routine procedure for post GCS women in a few years' time.
Sensitivity
Sex re-assignment techniques used until the 1980's placed no emphasis
on preserving and relocating nerves, as a result most patients had
little or no physical feeling in their clitoris, vulva or vagina.
Sexual stimulation was essentially mental, with little physical
reinforcement. The introduction of the penile inversion
technique was a vast improvement as nerves were preserved. The
latest techniques relocate nerves at the tip of the penis to the
clitoris, usually (but not always) resulting in excellent
sensitivity. Indeed, some transwomen now complain that their
clitoris is too sensitive, leading to problems in daily life, e.g.
when cycling.
Caveat Emptor - Buyer Beware You get what you pay for where SRS/GCS surgery is concerned, although the best surgeons and clinics in Thailand do seem to now offer better value than those in the USA, Europe and Australia.

Camel
Toe Pervesely, "Drag Queens" and transvestites now actively seek outfits that suggest a camel toe! (Right)
Surgical Advances
It's hard to underestimate the constant
advances in SRS/GCS surgical techniques. Like buying a car, next
year's model is always going to be better. Between the 1960's and 1980's only a handful of hospitals, clinics and surgeons around the world conducted SRS operations. Visually, the results were often brutal, with the vulva area having little resemblance to that of a natal woman. Pubic hair was used to conceal this. Photos of only the very best results - often after multiple revisions - appear in contemporary books and magazines. The 1990's saw the advent of celebrity SRS surgeons who tried to justify their high fees by pioneering new procedures such as colovaginoplasty, but complications were all too common. At least one follow-up revision procedure was generally required, e.g. to hood the clitoris.
The focus for new procedures has moved to the internal organs, in particular creating a vagina that doesn't require frequent dilation in order to achieve and then maintain depth. Another change is the pain resulting from the surgery. Ask any transwoman who had SRS before 2000 about her experience and she will recall in vivid detail the extreme pain she suffered in the week after surgery. Twenty years later some patients are more likely to discuss their desperate need for a shower!
Revision Procedures
Although many surgeons now advertise a "one step" SRS/GCS
procedure, the reality is that many women still have revision surgery,
typically a year after the primary surgery.
The second reason is cosmetic surgery to tidy-up and fine tune the
external appearance of the vulva. Even the most successful
operations through to the 1990's would now be considered "hachette jobs"
when compared to the external visual appearance of a natal woman.
In the 2020's, transgender women are seeking a textbook standard vulva
that few cis women have in reality!
Risks
Cancer Risk
Breast Cancer
Unlike men, a post-SRS transwoman faces the risk of cancer in her neo-vaginal tissues. This risk is greatly raised as the cells lining a neo-vagina slowly alter in type to that of a normal female vagina (technically a nonkeratinizing mucosal type squamous epithelium) - including normal vaginal PH levels, complete loss of hair, complete loss of pigment, complete loss of sweat glands, and normal vaginal epithelial glycogen levels. Medical evidence is still inconclusive as to extent to which the neovagina of a post-SRS/GCS transwomen takes on the characteristics of a "natural" female vagina. Whilst some medical studies have concluded that no significant changes in cell type actually occurs, clinics nevertheless find that the cervical smear test of a transwoman 10-20 years after SRS is often indistinguishable from that of a natal woman. Overall, the risk of cancer in the neo-vagina tissues of a post-SRS woman is probably very low. Nevertheless, having smear tests every 3-5 years should be considered as a pre-caution - particularly if there is a family history of cancer.
Cervical Cancer
Pelvic
Floor
Hymenoplasty
The 'First Time' After SRS, some transwomen want coitus as soon as possible, others might be reluctant but are under huge pressure from an over-eager male partner, whilst a few have become scared about the whole idea. A few tips for the first time with a man:
Almost no transwoman will orgasm the first time they have penetrative vaginal sex. A male orgasm is predominantly physically induced - it's centred on the ejaculation of sperm from his penis deep into a woman's vagina so that he can reproduce A virile young man may be able to orgasm again in as little as 15 minutes, but that increases to hours with age. By contrast, a female orgasm is essentially nature offering an incentive to encourage a woman to have intercourse with a man and get pregnant. It involves a mix of mental and physical stimulation - and as a bonus she can, unlike a man, enjoy multiple orgasms during a typical 5 to 10 minutes long period of penetrative intercourse. Also, again unlike men, a woman's ability to orgasm is unaffected by age, at least prior to menopause. In order to have an orgasm, a transwoman has to both adapt to and enjoy the physical stimulation of her new genitalia, whilst also developing her mental fantasies, e.g. having sex with a famous male hunk, or having sex on a tropical beach. Wearing sexy lingerie, dressing up, and even bondage may also help a transwoman in achieving that critical first ever orgasm as a woman. The active encouragement and help of her sexual partner is a wonderful aid where this is possible. Although not the romantic ideal, it's not unusual for the first orgasm post-surgery to be aided by a vibrator rather than a penis.
Regrets
C: "If
I had been properly assessed, it would have been obvious that sex-change
surgery was inappropriate for me, I was desperately unhappy and was
going for a sex change because I felt under pressure from my boyfriend.
I'll never have a relationship. Who's going to want me when they
could get a real woman? I am not a woman, I am a sex change, and
men know that. I fundamentally regret having had surgery. I
could have lived as a woman without mutilating my body, but no one
talked to me about the possibility."
M: "If and when you have [SRS] your life
will be forever changed, in more ways than you can possibly imagine and
anticipate. Being a woman is no better than being a man (in fact,
in many ways it's a lot worse) - you just have a new set of problems.
For me, being a woman expressed who I really am, but sometimes I think
the cost of that self-expression was too dear."
W: "Becoming a woman has been a disaster, this
experience has ruined my life. I felt excited when dressing as a
woman but looking back it messed up my head - [psychologists] had me
believing I'd always wanted to be one. [After SRS] I tried to
persuade myself I had no regrets. [A] reversal won't solve all my
problems, I will still be tortured by what I gave up to become a woman."
In the last case, Sam had SRS in 1997 to become Samantha, but reverted
to male in 2004 and had surgery to reduce his breasts and reconstruct a
penis.
Extra-ordinarily, in 2018 he decided that she preferred being Samantha
after all, and transitioned again and had another round of feminisation surgery! Over 21 years he/she spent £150,000 ($200,000) on
surgery.
The women's vaginas did not form properly while they were still inside
their mother's womb, a condition known as vaginal aplasia.
Current treatments normally involve surgically creating a cavity, which
is then lined with skin grafts or parts of the intestine - transsexual
women essentially undergo the same surgical treatment.
Under the new procedure a tissue sample and a biodegradable scaffold are
used to grow vaginas in the right size and shape for each woman - as
well as being an exact tissue match. After surgery, the woman all
reported normal levels of "desire, arousal, lubrication, orgasm,
satisfaction" and painless intercourse.
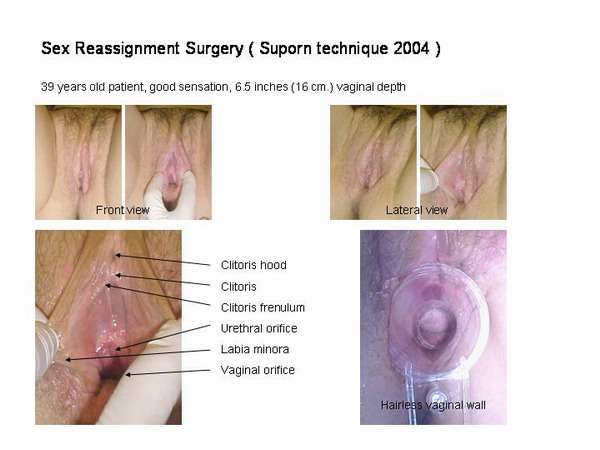
My Experience
After
a decade of prevarication and years comparing possible surgeons, I finally had
SRS/GCS (vaginoplasty) with
Dr Suporn Watanyusakulin. In the early 2000's he was receiving
glowing reports from many patients and had become a rival to top North
American surgeons such as Doctors Brassar, Meltzer and Biber, but
was a lot cheaper!
My recovery over the next week was sometimes very painful but it certainly wasn't the horrendous nightmare that
other women have reported.
Other than the small item of getting married, the next few months were basically letting my body heal and adjust.
My day seemed to be dominated by the boring routine of dilation. A highlight of my life happened about a month post-SRS. I went to take a
shower and, turning around, was surpised to see a naked woman. It took me a second to realize
that it was actually me
the mirror!
SRS
had re-located the nerve endings of my removed male genitalia,
concentrating them into my newly formed clitoris and vulva, with little
sensation in the vagina itself. My subconscious mind
was at first very confused and still associated
the nerve endings in my reconstructed genitalia with parts of my old
male anatomy. For example, several times I woke at night
needing to go to the loo and in a sleepy haze found myself standing over
the toilet looking for my penis!
About two months after
surgery my new husband gently explored my new female bottom
genitalia for the
first time and it was an uncomfortable feeling. When he touched my clitoris
I was certain that it was the glans of my penis, whilst when he
stroked my labia it was as though he was fondling my scrotum.
I reluctantly had to tell him to stop.
By six months post-SRS the scaring was fading and also being hidden by
pubic hair. I now had no doubt that I could pass visually pass as a woman
naked and even pass an intimate search by police or custom officers.
This immensely reduced the stress that I had felt since transitioning
what was now over four years earlier.
My
mind slowly reprogrammed itself and a year post-SRS I realised that my clitoris
now felt like ... well a clitoris.
Dr Suporn offered
me a follow-up revision procedure to resolve any issues from the SRS
procedure. I availed of this in 2006 and had minor surgery to "tidy up" and
improve the appearance of my vulva. This removed my final concerns about the appearance of my bottom.
My new normal was now being a woman - sexually, socially, physically.
But almost inevitably, there were problems. In particular
I had become susceptible to painful UTI's! And of course I
couldn't get pregnant, which became
crazily important when I got married. Even though most my friends and
family eventually knew that I was transgender, they assumed that my
biological clock was ticking and being in my late 30's I needed to
start
having children before it became too late. Many just didn't understand
the limitations of my surgery and kept giving me advice. It became really
depressing knowing that there was no chance that one day I could
announce "I'm having a baby!".
I'm now 20 years post-SRS/GCS and have no regrets other than wishing that
I'd had undergone the surgery ten years earlier.
Note: I discovered in 2005 that Dr Suporn was using photos of
me on his website and in medical papers, upon enquiry I found that I had signed
documents giving him the required permission. This is apparently a common clause
in surgery consent documents. However. the fact that photos were probably taken
before, during and after surgery may be relevant for patients that
have poor results or suffer from complications.
More Information
In 2013 I completed a survey conducted by Transgender
Equality Network Ireland (TENI), the resulting
report is
worth reading and I suspect that other Western European countries will
have very similar results.
For the very interesting results of a Post-Operative Survey of transsexual women, see
here.
For a dire warning about the risks of low cost, back street SRS, read this
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
(c) 2000 - 2024 Annie Richards
Please send any comments, feedback or additions to:

Last updated: 1 April, 2023

 It is important not to romanticize SRS/GCS. It is brutal, major,
painful and expensive surgery that involves permanent male castration and
infertility, the removal of an often-functional penis, and the creation of
a vulva and high maintenance vaginal cavity that imperfectly attempts to
mimic cis-female sexual organs, with a loss of sexual libido, enjoyment
and the ability to orgasm also likely. And on top of this is the risk of
serious immediate or long-term
medical complications.
It is important not to romanticize SRS/GCS. It is brutal, major,
painful and expensive surgery that involves permanent male castration and
infertility, the removal of an often-functional penis, and the creation of
a vulva and high maintenance vaginal cavity that imperfectly attempts to
mimic cis-female sexual organs, with a loss of sexual libido, enjoyment
and the ability to orgasm also likely. And on top of this is the risk of
serious immediate or long-term
medical complications. 




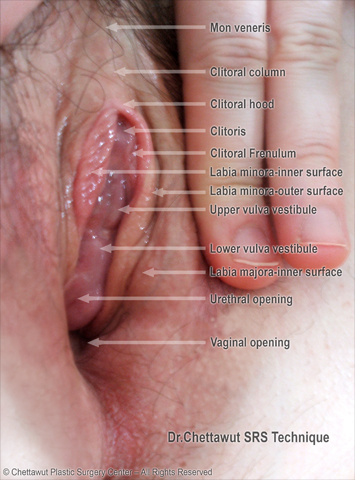
 A
natural appearing
vulva (external 'bottom' genitalia) including mons pubis, labia minora and majora
A
natural appearing
vulva (external 'bottom' genitalia) including mons pubis, labia minora and majora 









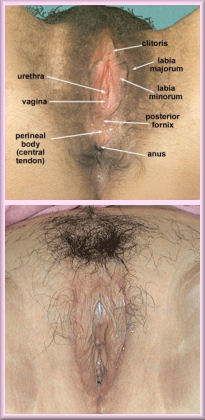

















 A common problem for all women is that when wearing panties or a
bikini, the fabric can be sucked into their vagina, leading to what is
called a 'camel toe' appearance. Post-SRS transwomen are
particularly susceptible to this problem as their vulva entrance is less
protected by surrounding tissues, particularly if they haven't had a
procedure to hood their clitoris. As such a regular 'camel toe'
has become an outing indicator, and ironically tucking when pre-SRS can
result in a better female appearance when clothed!
A common problem for all women is that when wearing panties or a
bikini, the fabric can be sucked into their vagina, leading to what is
called a 'camel toe' appearance. Post-SRS transwomen are
particularly susceptible to this problem as their vulva entrance is less
protected by surrounding tissues, particularly if they haven't had a
procedure to hood their clitoris. As such a regular 'camel toe'
has become an outing indicator, and ironically tucking when pre-SRS can
result in a better female appearance when clothed!













 Back to Articles
Back to Articles