(Part 1)
![]()
|
Important Update On 28 July 2022 the UK's NHS announced that it was
shutting
down the Tavistock Centre transgender clinic after a review found that it was “not safe” for children.
By the late 2010's children referred to Tavistock were often receiving just one short assessment, at the end of which transition was usually recommended to the parents. Puberty blockers were prescribed to many of the children - the clinic reported 40% in a 2011 medical paper (some as young as 10), but anecdotally this increased considerably thereafter. Unmonitored hormone treatment would then automatically follow when the child reached age 16 (and often much younger if requested), and finally gender confirmation surgery when 18. Whilst the Centre's emphasis on the provision of interventionist medication and surgery at a young age had worked well in the early 2000's - and indeed still immensely benefited a small minority of the young children that it treated - it was unfortunately unsuited to the avalanche of referals now being received. Parents started to push back against the radical treatments that were being recommended for their child after only a minimal consultation. This was given credibility by investigators finding that many of the referred children (37%, but up to 64% if children that the clinic lost contact with are included) were reverting to their cis-gender before having GCS, whilst many who did have surgery soon bitterly regretted what had been done to them. This sorry saga shows the vital importance of thoroughly assessing a child who identifies as transgender, and then continuing to track their mental state before any irreversible medical treatment is performed.Given the events at the Tavistock Centre, some of the statistics quoted in this article hould now be taken with a large "pinch of salt" as to their real accuracy. |
Introduction A major challenge since c.2010 had been the explosion in the number of children who suddenly identify as being as being transgender as a teenager - which overwhelmed the UK medical system. I struggle to find the numbers credible (over 1% of all teenagers) and agree with those that suggest that it is a "blip" based on social trends that may soon reverse. The priority for the medical system should be on the far fewer (one in several thousand) but consistent number of transgender children who display symptoms of Gender Identity Disorder (GID) in early childhood. Typically a transgirl wants to play with toys and wear clothes traditionally used by the opposite sex by age 2-5, and starts to insist that she's a girl, not a boy.
When allowed to, such children are almost always able to rapidly and successfully assimilate themselves into society as a female, this alone is enough to differentiate them from the experience of most transsexual women who transition when an adult.
Prevalence
Meaningful statistics on the prevalence of transgender children only began to be collected in the late 1990's. Textbooks published before then commonly state that about 1 in 10,000 children have GID, this number seems be based on a single study made in the 1970's.
Note: The figure of 600 excludes the very small proportion of "XY" intersex children born in the UK with ambiguous or malformed genitals who are assigned to the female gender by doctors while still a baby, perhaps 20-40 each year deriving from USA figures. There are also many children with "male" genes who are identified at birth as female and then brought up as girls, for example there are perhaps 3000 "XY" women in the UK who were born with Androgen Insensitivity Syndrome.
By the early 2000's the UK's NHS was suggesting that 1 in 4000 children was transgender, the Netherlands and Belgium 1 in a 2000, whilst the number in some Asian countries was reaching 1 in 500 (almost all Male-To-Female).
The newly launched UK Charity Gires had a sceptical reaction when it claimed in 2010 that there were now 26,000 "young people" in the UK with gender identify problems, and that the number would soon reach 100,000, i.e. about 1 in 130 of the UK's population under age 18. However, in 2016 the UK's NHS website was suggesting that 1 child in a 100 had gender problems, supported by reports from secondary schools which showed that nearly 1% of students age 11-16 were being registered either by the student or their parents as having GID. Presentations by company HR Managers at conferences again support this percentage for new employees age 16-22. A study of 8000 students in New Zealand also arrived at a figure of less than 1 in a 100. The growth in the number of transgender children in the UK can be illustrated by the exponential growth in referrals (of all ages) to the Tavistock and Portman NHS Foundation Trust in London - which used to be the primary UK centre for children and adolescents with GID:
The UK is far from unique in seeing an upward trend. The chart below compares the UK's experience with Australia, their respective populations in 2019 were 67 million and 26 million so the relative difference on the linear trend rates is small.
Similarly, in 2015 Fenway Health, a highly respected LGBT focused clinic based in Boston (USA) that was founded by local university students published the following graphic showing the extraordinary growth in the number of transgender patients that it was treating:
By 2021 the number of transgender patients being treated by Fenway was over 4,400. Although its transgender patients are generally "particularly young", since at least 2020 the clinic has been seeking to better support "older adults".
The balance has also changed from female-to-male (FTM) children greatly outnumbering female-to-male (FTM), to the exact opposite - the Tavistock clinic now has more than two FTM referrals for every MTF. The referral of young people assigned female at birth (AFAB) to NHS gender clinics now outnumber male at birth by more than two to one, although among adults the opposite is still true. One study estimates that "just" 2-6% of natal boys exhibit cross-gender characteristics, compared to 5-12% of girls.
Sex and Gender A person's sex and gender can be determined or judged by many factors, including:
It is quite possible for these factors to disagree and contradict, e.g. a post-operative transsexual person may have a male birth certificate, a male karyoptype (XY genes), no internal female sex organs, female appearing genitalia and secondary sexual characteristics, live and identify as a woman, but be sexually attracted only to other women and in a lesbian relationship. Factors 6, 7 and 8 are commonly and unfortunately combined under the term "gender-role", but I prefer to keep them separate when possible. A particularly confusing but frequent use of the word gender is in the phrase "Gender Re-Assignment Surgery" (GRS). It's essential to differentiate between a person's physiological sex (factors 4 and 5), and a person's social & mental gender (factors 6 and 7), surgery can't ever change the later and phrase "Sex Re-Assignment Surgery" (SRS) is a better, although still seriously exaggerating, description of what surgery can achieve.
Gender For most children their legal, chromosomal and physical sex agree with their mental gender and preferred gender role.... but not always. As already mentioned, children with gender identity problems are described as having gender dysphoria.
Establishing a gender identity is a process that most people take for granted, but that no one completely understands.
Scientists and sociologists agree that traditional gender roles are in many ways socially constructed, e.g. girls learn to wear dresses and boys learn to wear trousers. But no one seems to understand what makes a transsexual child raised in a male gender role embrace the female role as her own and vice versa. Nor can anyone explain why many intersex children raised as one sex eventually migrate back to the gender that their genetics or their prenatal hormonal environment would have predicted.
Bill Summers, a professor of medical history at Yale who has studied the science behind gender and sexuality says "You have to learn somehow what it means to be a boy or a girl. You don't come born with this idea. But enough people say, 'I always knew I was a boy but I was raised as a girl' that I can't doubt they have these feelings."
The bottom line seems to be that sociologists and psychologists still don't know where gender identity comes from or why - but it is unlikely that either biology or society operates totally independently from the other. The only current certainty seems to be that when a young child decides that they are a boy or a girl and this decision contradicts their supposed physiological sex, the result is much anguish and cost to the child, the parents and the medical profession.
Physical Appearance
From circumstantial evidence it's
long been suspected - even assumed - that the physical
appearance of early transitioners is skewed towards their
preferred gender. However there has been very little
formal research on this, one of the few medical papers I have
found is the
Physical attractiveness of boys with
gender identity disorder
by Zucker et al, which
dates to 1993!
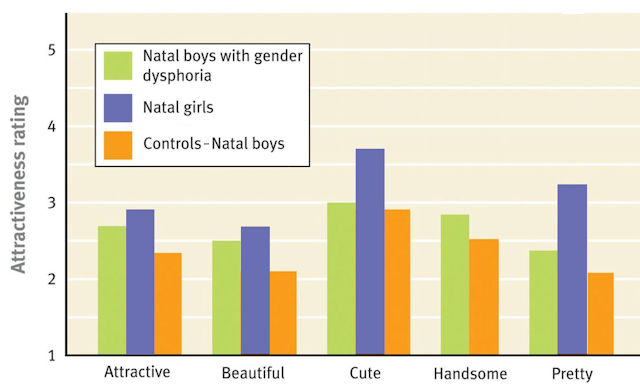
In this study,
36 university students blind to the actual sex and gender of the
participants rated 17 boys with gender identity disorder (GID), 17 clinical control boys,
and 17 natal girls regarding their physical
attractiveness. Ratings on a scale of 1 to 5 were made of the
face and upper torso from photographs taken at the time of
clinical assessment (mean age, 8.1 yrs).
On all five objectives (attractive, beautiful, cute, handsome,
and pretty), boys with GID were judged to be more attractive
than were the clinical control boys, but less attractive than
the natal girls on the four objectives that the later were rated
on.
Natal cis-girls were not evaluated in the category
of "Handsome, it is not explained why. The difference between the GID boys and the
girls under the categories Cute and Pretty is statistically
significant, with little overlap between the two groups.
Boys raised as Girls Whilst the practice is far rarer in the West, it does happen. Dr Money and his colleagues may well have been influenced by encountering patients who had been bought up and now considered
themselves to be of a gender that was different from their physical sex. A recent (2019) and high-profile example is the actress Meghan Fox who is allegedly encouraging her three young step-sons to live as girls.
Meghan regularly posts photos of her sons wearing dresses, stating that
"Noah started wearing dresses when he was two". She began to teach her kids about gender
equality when her eldest son Noah started wearing dresses at the age of two,
stating "you can be a boy and wear a dress. In 2021 she implied that all
three of the boys (then aged 5, 8 and 9) had transitioned, but caveated this by saying "You
can express yourself through your clothing however you want and that
doesn't even have to have anything to do with your sexuality.
Press reports in February 2024 confirmed that all three children
identified their gender as female and were living as girls. It's probably just fun for them
pre-puberty, but the odds are still that they grow up to be
cis-men.
Gender
Identification of Transsexual Children
A result of John Money's pioneering work in the 1960's was that the sex re-assignment of babies and very young boys became medically acceptable in the 1970's and 1980's, and with hindsight far to common as up to two-thirds of patients eventually rejected their assigned female gender. Early re-assignment and surgery then became rightly discredited, but unfortunately there has been a carry-over affecting young transgender children in the age 3 to puberty range.
Whilst there is no such thing as the typical young child with GID, perhaps a good example is Zach Avery. At first, he seemed to be a 'normal boy' but when age 3 he turned around and told his mother, Theresa, "Mummy, I'm a girl". She assumed that he was just going through a phase and just left it at that, but Zach started to insist on wearing his sister's clothes and would become upset if anyone referred to him as a boy. Theresa notes that "He used to cry and try to cut off his willy out of frustration". His parents became increasingly worried by Zach's behaviour and took him to the doctors. After numerous consultations and observations, he was officially diagnosed by NHS specialists as having GID, and transitioned age 4. A key, if obvious, differentiator between transsexuality emerging in children and the far more numerous instances of it emerging in an adult is the pre-puberty age at which noticeable cross-gender behaviour appears in the former group. This has been confirmed by numerous studies.
In one study, two thirds of transsexual boys were aware that they belonged to the opposite sex and exhibited such behaviour by age 5, and 77% by age 10. Another study of 137 MTF transsexuals, 70% exhibited cross-gender behaviour before age 10, and another 20% before age 15. A third study of 121 transgender individuals between age 18 and 65+ gives a modal average of 5 years for the age when the participants began to question their assigned gender, and a mean average of 7.9 years. Just 4% first had doubts about their gender after age 18. Over 80% of the participants in the study were assigned male at birth.
It seems that until the 2010's most young transsexuals suppressed their doubts about their assigned gender, as one later said "my overriding need was to a keep it quiet and not come out and seek acceptance that 'God has made a mistake'". But there were brave exceptions. For example, Richard ('Richie') always wanted to wear dresses like his sister, when age two and a half his mother caught him trying to cut his penis off with nail clippers, saying "this doesn't go here". At age 7 he was finally diagnosed as having Gender Identity Disorder, his parents changed her name to Riley Elizabeth and let her go to school as a girl - where she blossomed from a "sad confused little boy into a happy young girl". The financial burden of Riley's medical care had been crippling, but her parents had no doubts - "seeing Riley's happy face now, it's worth every penny".
The story is very different for boys diagnosed with gender dysphoria when around puberty. Several studies since 2010 suggest that more than two-thirds eventually accept that they are actually male when post-puberty, only 18% eventually have female GCS as female - and many of those soon regret it. This opens a host of questions about the amount of medical support that they received, their access (or lack of) to puberty blockers and hormones, an inability to transition, social and family pressures, sexual orientation, and the long term physical and mental consequences - particularly on those girls still diagnosed with gender dysphoria.
The inevitable result of these problems is a general reluctance by the medical profession to supportively treat a physically normal boy with gender identity problems. It again seems too often require courageous and forceful parents before a doctor will medically facilitate the transition of a minor.
Parents
It is impossible to underestimate how important the understanding and support of parents is for a young transsexual her eventual success in life. It is also difficult to underestimate how much emotional strain having a transsexual child can impose on his/her parents. Many parents become a pillar of support and understanding, indeed there are many instances of parents going to extraordinary lengths and expense to aid their new daughter - for example moving house so they can go to a different school and avoid anyone who knew them as a boy. In another positive example, Jamie never felt herself to be a boy, and when at age 11 she finally told her parents "You think that I am a boy, but I am a little girl!", they accepted her choice and she is now living very happily and confidently as their daughter.
On the other hand, there are also instances where the child tells the parents and the result is a nightmare of arguments and pressure. Rachel (formerly Daniel) describes how when she told her parents at age 17: "They didn't shout at me but the conversation was very heated. Mum got upset - although she said she'd guessed a while ago - and Dad was annoyed. They both said they didn't want me to dress up in the house and that I'd always be Daniel to them. ... My parents have been good to me, but they'll always see me as their son."
Rachel is actually luckier than many girls. Enforced visits to a suitable psychiatrist (suitable for the parents at least) to treat the child's gender disorder are common. Perhaps in a few cases a "cure" is achieved, but more commonly the child suppresses his/her transsexuality, and if he persists then an eventual total rejection by one (usually the father) or even both parents may well occur. For example, Brazilian Roberta Close was disowned by her father, and only reconciled years later. While now a successful model and actress, for several years in her teens Roberta descended into the seedier side of life that all too many transsexual women go through in order to earn a living.
Often transsexual children feel unable to tell their parents
about their feelings and needs. This usually means that a public
admission of their transsexuality is deferred to adulthood - and the delay
is always much regretted. But also the resourcefulness of children
should not be underestimated. For example, one textbook (Man and
Woman, Boy and Girl) describes how a woman secretly obtained and took
hormones while still a young teenage boy. Her concerned parents
eventually took her to hospital for tests to help determine the cause of the
resulting physical changes, but she had had enough warning to stop and let
her system clear. The doctors concluded that the changes were
spontaneous and natural (some degree of gynaecomastia - male breast
development - is quite normal in mid-puberty boys), and told the parents not
to worry.
Guidelines for the Treatment of Transsexual Children
Although still not coming out in favour of starting feminizing hormone treatment at a normal puberty age and delaying any sex change surgery until at least age 18, the standards do at least now allow the treatment of very young adolescents with puberty-delaying hormones and thus help prevent the socially and mentally disastrous development of normal male [secondary] sexual characteristics and appearance in an under-16 MTF school girl. In a best case this now allows age critical medical treatment to stop male characteristics developing, but female sexual characteristics optimised by early hormone treatment are still banned. In its defence, the "Standards of Care" is clearly and understandably concerned about some instances of unsuccessful boy-to-girl gender re-assignment of intersex babies, such as the highly publicised failure of the gender re-assignment David Reimer (aka the "John/Joan" case), and wants to avoid any future repetition.
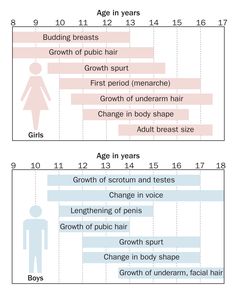
Puberty is often a nightmare for 'gender dysphoria' children according to Cohen Kettenis, Professor of Psychology at the Medical Centre of the Free University in Amsterdam, "They develop an enormous dislike for their body." Most children seen by Professor Cohen react with horror to the changes that occur in their bodies at puberty. It appears that their so-called "transsexual" feelings become much stronger and they do not feel at home in the body that they now developing. Margaret Griffiths of the Mermaids support group says very similar things, "Some girls and boys go through Hell at puberty, they have few friends, they are bad in the school, because they can concentrate on nothing, and some have suicidal thoughts."
When - at age 10 - Riley (who had been living as a girl since age 7) was warned by her mother that nature would soon start turning her in a man, her reaction was a horrified "Please don't let that happen ... please!". Although the child may not admit to his transsexual desires at this stage, the parents will often start to have some concerns about their son. The onset of puberty is a critical point as the child is faced with his own undesired physical masculinisation, often combined with a great jealously of girls and their physical changes, by age 15 some 90% are exhibiting feminine behaviour. This is the point where many transsexual children finally admit to their wish to be a girl and they, or their parents, seek help.
Zoe, age 21, concurs about puberty: "When puberty arrived I was repulsed by my erections and deepening voice. At times I felt suicidal." Jamie Cooper was 12 when she wrote her mother a letter saying that she should have been born a girl, they sought medical advice and were told that it could just be puberty, the feelings deepened but she had to wait until she was 16 before receiving hormone treatment - she transitioned on her 16th birthday.
A lot more information about puberty and its effects is given in the
separate
article here.
Professor Cohen's policy is that if it appears that the gender dysphoria feelings are becoming stronger, then they should be prescribed puberty blockers to temporarily halt puberty until they are 16. When they are 16 and quite certain that they have the wrong body, they can be prescribed hormones as well as to begin to change their outward appearance to more closely match their chosen sex, "After that comes the actual sex-change operation".  A photo from 2021 showing four Australian transgirls, from the left Grace Hyland (age 21), Evangeline Macdonald (age 17), Belle Bambi (age 23) and Avery Clemens (age 25). They began taking female hormones or puberty blockers at ages 18, 10 (blockers), 13 (blockers) and 18 respectively. (Australia)
T Even if it not possible to begin female hormonal treatment before a male puberty has commenced, the results can still be remarkable results if started whilst the body is still at its most receptive age - the critical puberty years between about 11 and 17 (depending on the individual), but the earlier the better. It is no coincidence that so many transsexual women who are famed for their looks had begun taking hormones by 17 - Jenny Hiloudaki, Tula, Hari-su, Roberta Close, Dana International, etc.
Doctors certainly seem to agree that giving - for example - a 13-year-old transsexual boy-to-girl doses of oestrogen will make her physically far more attractive as an adult woman. However they also agonise about the possible negative consequences - and perhaps their potential legal liabilities from prescribing female hormone to "boys".
The treatment model developed for intersex children born with male testes but assigned as female is very relevant young transgender MTF children. In order to maximise physical feminisation, low level oestrogen treatment of the young intersex girl begins at age 8-9 years. Before the onset of a natural puberty a bilateral orchiectomy (castration) is performed age 11 to remove the testes and hormonal treatment is then increased (additional oestrogen, later supplemented with progesterone) to initiate a female type puberty.
When an orchiectomy is performed before puberty, the results in terms of increased physical feminisation and decreased masculinisation are much more dramatic than when it is done after puberty.
Puberty Blockers The 2010's have seen a huge increase in the number of apparently transgender children, but anecdotal reports indicate that up to a third change their mind within a year of transitioning. Many Western doctors are thus very reluctant to
perform any irreversible surgery, or even prescribe feminising
hormones, for a transgender child under age 16. Instead,
they often prescribe GnRH
agonists or
analogues (commonly known
as 'puberty blockers') such as
Goserelin Acetate (commercially sold as Zoladex) and
Leuprolide Acetate
(sold as Lupron). These prevent
or dramatically reduce gonadal hormone production, including
testosterone, thus preventing the onset of the masculinising changes
of adolescence. The
drug is usually delivered via a weekly or monthly
subcutaneous injection into the abdomen.
While the treatment does nothing to directly promote female physical
characteristics in the girl, it does prevent or greatly slow male
type puberty with its physical effects, and several Dutch studies
have confirmed the effectiveness of such treatment. As
mentioned above, it's been discovered that some GnRH
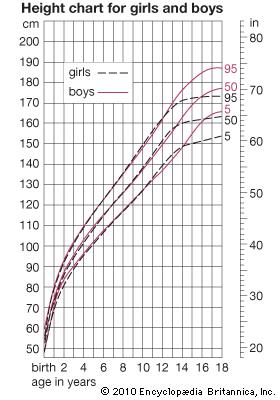
agonists help trigger a female puberty in a transgirl. Puberty blockers apparently have the important advantage of gaining time whilst the transgender child considers and reconfirms their choice of gender. Another big advantage of blockers for a boy-to-girl is that they don't have to start taking a high dose of oestrogen whilst pre-teen. An 11 or 12 year old boy is actually shorter than the average girl of the same age, and starting oestrogen therapy at that age may restrict their height to under 5ft (about 151 cm) - very short even for a girl. Obviously every transgirl is different but delaying oestrogen treatment until age 13 or 14 is likely to result in an average female height, whilst 15 may result in an above average height for woman, but not excessively so (i.e. ideal for a model). Unfortunately GnRH analogues are expensive drugs, but they are to be much preferred in adolescents over the cheaper anti-androgens such as Aldactone (Spironolactone) and Proscar (Finasteride) which are commonly prescribed to post-puberty transsexual women, but which are increasingly suspected of having unwanted side effects, including reduced breast growth.
By 2010 the UK's NHS had become one of the most progressive medical organisations in regards to the treatment of transgender children. Doctors are now prescribing puberty blockers from age 10 and hormones from age 12. Unfortunately, because of the John/Joan case, and mistakes made in the past when dealing with intersex children, recent medical studies have tended to emphasise the minority (about one quarter) of gender disordered children who don't eventually have SRS, and the disadvantages of early gender and sex-role re-assignment. In particular, many advise against early genital surgery or irreversible feminising hormonal treatment. But they neglect to consider why so many young transsexuals eventually have SRS despite the immense "corrective" pressures often exerted on them, nor do they consider whether those that don't have SRS would have perhaps enjoyed their lives more as a woman than they now are as a man.
Nevertheless, many gender clinics seem to be moving the earliest age for the prescription of hormones rather than puberty blockers to transgender children from age 18 to age 16. All the accumulating evidence is that the earliest possible hormonal treatment has significant physical and mental advantages - even compared to puberty blockers.
1. Boys tend to start puberty later than girls. It is very unusual for a boy to be prescribed puberty blockers until age 11 or 12, by which time most girls are several years into their puberty. 2. Puberty blockers stop the development of male secondary characteristics but they don't stop the clock. The human body seems to be fundamentally geared for dramatic sexual development between ages 10 and 15. Stopping blockers and beginning female hormones when age 16 is simply too late, the frequently disappointing breast development of many such girls who start taking oestrogen in their late teens is strong evidence of this.
Doubts Emerge About Blockers Around 2020 serious doubts began to emerge in the UK and elsewhere about the widespread prescription of puberty blockers for young teenagers. In the UK these were being prescribed to thousands of children between ages 10 and 15 on the basis of a single cursory (often just 10 minutes long) clinic and assessment. Whilst blockers prevent the development of physical secondary sexual characteristics, they don't prevent the general aging and development of the body. If blockers are ceased after a few years, the patient's body (and mind) won't miraculously bounce back to a state equating to that if they had never been taken. Instead, problems such as reduced libido and fertility are very likely. It's become clear that puberty blockers are not a panacea and instead create new problems, as such their prescription has greatly reduced in recent years.
If a boy is diagnosed as a transsexual then a failure to immediately start treatment is not only deferring the inevitable in the vast majority of cases but is doing so at a considerable cost to the child's future as a girl and woman. It's indisputable that the earliest possible transition and pre-puberty hormonal and surgical treatment will offer most boy-to-girl's massive psychological and physical benefits.
An example of this is Ariel Nicholson Murtagh. He knew from a very young age that he was actually a girl. Her mother, Kerry, was very supportive and battled for his right to transition and receive medical support. [Sadly her father was far less supportive, and this was a major factor in the marriage ending.] When age 10, his mother let her transition and change her name to Ariel, she also began injections of Lupren to suppress her puberty and prevent her voice from breaking. In 2015, age 14, she appeared in the PBS documentary “Growing Up Trans”, talking with a therapist from the Ackerman Institute about wanting to take oestrogen. She finally started taking hormones age 15. The PBS documentary resulted in her being discovered as a model, her first catwalk was for Calvin Klein in September 2017, in 2018 the influential models.com website added her to their "Hot List".
Another example of the results of early medical treatment is Wyatt and Jonas Maines. They were born identical twins, but from a early age Wyatt rejected being a boy. His parents were very supportive, and at age 11 the twins became brother and sister when Wyatt transitioned and changed her name to Nicole. The family sought medical help from the Children’s Hospital Gender Management Services Clinic in Boston, USA. The clinic prescribed Nicole with puberty blockers and female hormone injections. The dramatic effect of this treatment is shown by the fact that at age 14 Jonas (in mid-male puberty) was 167 cm tall (5ft 6 inches) and weighed a 52 kg (115 pounds), whilst Nicole was still a petite 155cm (5ft 1inch) and weighed only 45kg (100 pounds).
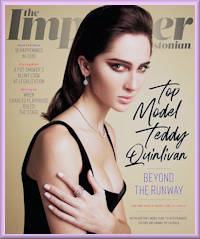
Supermodel Teddy Quinlivan, risked her career when in 2017, age 24, she decided to tell a CNN reporter that she was transgender. She emphasised that her success as a female model was due to transitioning and beginning hormones at a young age:
A recent follow-up study of sex-reassignment in 22 adolescent transsexuals (ten started hormones under age 16, twelve under 18) found that post-operatively in all cases all signs of gender dysphoria had disappeared, they scored normally in psychological tests and they were socially functioning well. Not a single girl/boy expressed feelings of regret concerning their decision to undergo sex reassignment. The study concluded that with careful preliminary screening, starting sex reassignment procedures before adulthood results in favourable post-operative functioning. Advantages of Early Hormone Treatment
Early hormone use (i.e. during puberty) in a trans-girl allows a typically normal female body shape to develop, with significantly more fat and less muscle than otherwise, the girls post-puberty body shape and "figure" will become far closer to female than male norms in its proportions. For example, a 2021 study claimed that the development of hip bone geometry during gender-affirming hormone therapy in transgender adolescents resembles that of the target gender if hormone treatment is started in early puberty. The details of the study are not fully supportive of this headline but do suggest that a transgirl starting hormones by age 14 is likely to have after puberty a pelvic girdle half way between male and female averages.
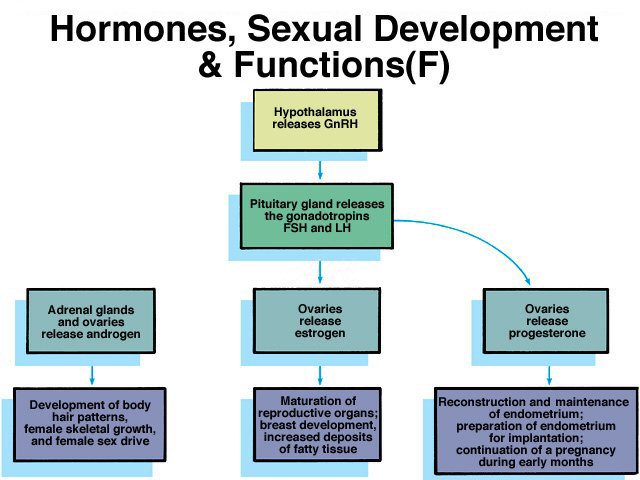
In general, increased levels in the blood plasma of oestrogen and progesterone will stimulate and promote the growth of female secondary sexual characteristics (breasts, fat distribution, pubic hair pattern, ...) while the reduction in the levels of androgens such as testosterone will, if early enough, completely prevent the development of male ones (deepening of voice, facial hair, muscular development, ...). F Maximum possible feminisation occurs if hormonal treatment begins before a male puberty would have start started. Very conveniently, girls tend to start puberty two years earlier than their male peers, so high dose hormone therapy intended to initiate a full female type can be safely started by age 11, although it in practice it is often deferred to 12 or even later, particularly if the individual's physical development allows that. If her testes were removed in infancy or childhood, then for health reasons low level hormone therapy should be begun by age 9 - an age at which many girls begin to notice some initial puberty changes, in particular the development of breast buds.
An
example of the disadvantages of no early hormone treatment is
Jenny Maquir (right)
who was born in 2001. By age 6 she knew that she was a girl, not a
boy. Unfortunately she lives in Ireland and the health service there
has almost no capacity to treat children with gender identity issues.
GnRHa pubertal induction
An important development since 2000 is the discovery that gonadotrophin-releasing hormone agonists (GnRHa) such as Leuprolide (sold as Lupron) can help trigger the onset of a female puberty in transgirls when combined with estrogen hormone therapy, usually Estradiol. As a "puberty pulse" generator it's typically taken as an intramuscular injection every six months - as few as two injections may be prescribed. The resulting visual body feminisation is significantly greater than from estrogen alone. Results After reading hundreds of reports, case studies and personal blogs, I’ve concluded that if a transgirl starts puberty blockers by age 11 and oestrogen hormones by age 14 she will have a female type puberty. The likelihood of her then being misidentified as male is almost zero. For more information, I recommend a reading of the 2020 medical paper Assessment and Hormonal Management in Adolescent and Adult Trans People, With Attention for Sexual Function and Satisfaction With Attention for Sexual Function and Satisfaction, by T'Sjoen G, Arcelus J, De Vries ALC, Fisher AD, Nieder TO, Özer M, et al. This essentially is a collation of many small medical studies, and it identifies the following key results in transgirls taking gender confirmation medication:
In a genetic girl, her increasing production of oestrogen
during puberty causes her skeleton to mature so that growth eventually
stops. Oestrogen treatment can speed up this bone maturation by
accelerating the completion of growth in the growth plates (the zones of
growing cartilage near the ends of children’s bones) and thus suppresses
growth somewhat, by up to two inches. Paediatric endocrinologists
sometimes prescribe large doses of oestrogen (usually Ethinyl Estradiol) for
a period of several years to deliberately restrict growth in excessively
tall girls.
The same technique can theoretically be used to help induce in a young transsexual girl a final height of 63" - 69" - typical for a Western European woman in the early 21st century. However, obtaining supervised treatment to restrict the height of a transsexual boy-to-girl to female norms is very difficult as height is not considered to be a disease. Endocrinologists are reluctant to treat even a genetically female "XX" adolescent unless bone growth X-rays show that excessive adult height for a female (over 71") appears likely.
The Brain
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Last updated: 29 November, 2018
|
Formerly the "Birth of Venus"
(c) 2000-2025 Annie Richards |




 In 1997 Press for Change reported that in the UK
there were 600 transitioned
In 1997 Press for Change reported that in the UK
there were 600 transitioned
 However,
since 1997 the recorded number of transgender children has exploded.
New sources of information such as the internet and TV documentaries
mean that children and parents are no longer accepting as gospel the
advice of an experienced and over-loaded doctor or psychiatrist.
The growth in reported GID cases among
However,
since 1997 the recorded number of transgender children has exploded.
New sources of information such as the internet and TV documentaries
mean that children and parents are no longer accepting as gospel the
advice of an experienced and over-loaded doctor or psychiatrist.
The growth in reported GID cases among  A UK study
published in November 2005 said that there were 2,000 young
transsexuals in the country age 15-19, about 1 in 2,500 of that age
group.
A UK study
published in November 2005 said that there were 2,000 young
transsexuals in the country age 15-19, about 1 in 2,500 of that age
group.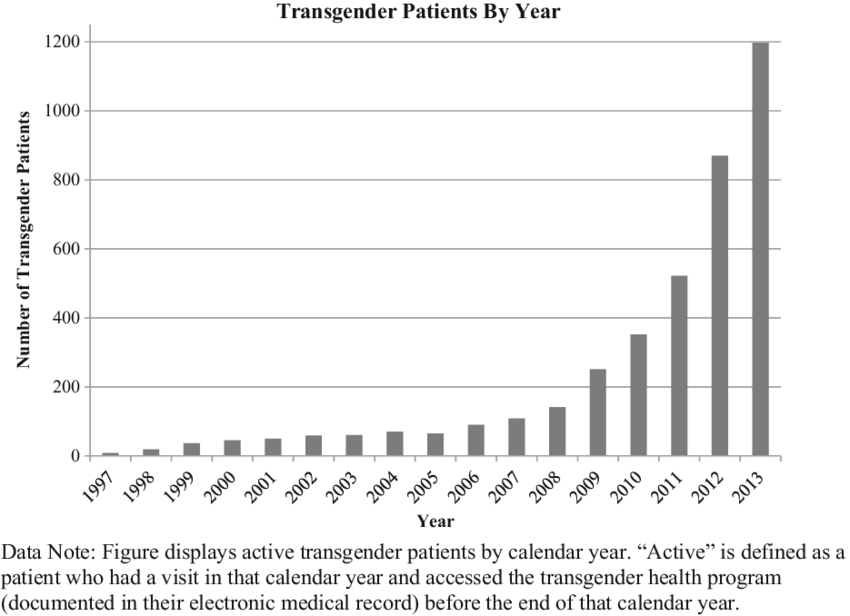
 The
UK's NHS reported that the average (mean) age of patients being
referred to its gender identity clinics in 2013 was 42. In 2015 it
was just 30 after
repeated huge annual rises in the number of teenagers with gender
disorders - the Sun
newspaper
The
UK's NHS reported that the average (mean) age of patients being
referred to its gender identity clinics in 2013 was 42. In 2015 it
was just 30 after
repeated huge annual rises in the number of teenagers with gender
disorders - the Sun
newspaper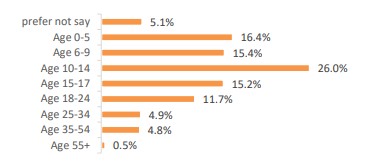
 With
the increasing awareness and more favourable publicity given to
transgender, MTF children who in the past would have suppressed
their female gender, or at least defer dealing with it openly until
reaching adulthood, are now coming forward while still a child.
In most cases their families respond very positively and
supportively, but occasions of outraged parents and internal family
battles about how to deal with a would-be daughter will never cease
completely. Perhaps a good indicator of the changed situation
is that by 2016 about 90% of UK primary and secondary schools had
policies to support transgender students.
With
the increasing awareness and more favourable publicity given to
transgender, MTF children who in the past would have suppressed
their female gender, or at least defer dealing with it openly until
reaching adulthood, are now coming forward while still a child.
In most cases their families respond very positively and
supportively, but occasions of outraged parents and internal family
battles about how to deal with a would-be daughter will never cease
completely. Perhaps a good indicator of the changed situation
is that by 2016 about 90% of UK primary and secondary schools had
policies to support transgender students. There
continues to be a reluctance by the general medical profession to
pro-actively treat gender identity disordered children. In the UK a
referral to the few specialist NHS clinics is the best outcome,
although these are being overwhelmed by numbers that are roughly
doubling every year. It is also worth noting that young
transsexuals (i.e. under age 20) seeking and obtaining medical help
and treatment at these clinics are still vastly outnumbered by their
older counterparts - most of whom bitterly regret their years of
delay. But a major problem is that the NHS's waiting list for
GID treatment is two years, and additional resources are desperately
needed. There is strong case that younger transgender patients
should be prioritised over older patients - unfair though this may
seem to the later.
There
continues to be a reluctance by the general medical profession to
pro-actively treat gender identity disordered children. In the UK a
referral to the few specialist NHS clinics is the best outcome,
although these are being overwhelmed by numbers that are roughly
doubling every year. It is also worth noting that young
transsexuals (i.e. under age 20) seeking and obtaining medical help
and treatment at these clinics are still vastly outnumbered by their
older counterparts - most of whom bitterly regret their years of
delay. But a major problem is that the NHS's waiting list for
GID treatment is two years, and additional resources are desperately
needed. There is strong case that younger transgender patients
should be prioritised over older patients - unfair though this may
seem to the later.  Young transgirls tend to immediately and
successfully go
Young transgirls tend to immediately and
successfully go 



 Summers points to the work of Dr John Money who became famous in
the 1960s for recommending and surgically facilitating the
transition of a young boy (Bruce Reimer) with a botched circumcision into living as
a girl (Brenda) from age 17 months - medical studies changed the
names and it became know as the "John/Joan" case. Dr Money declared
when Brenda was age 9 that the gender re-assignment was a complete success.
However, this finding was
undermined when Brenda grew up with a masculine gender
identity anyway, and eventually decided to live as man, choosing the
name David. Summers notes that "the whole idea [was] that
given hormone treatment and the right social environment, you can
determine gender identity. It's not really quite so simple."
Summers points to the work of Dr John Money who became famous in
the 1960s for recommending and surgically facilitating the
transition of a young boy (Bruce Reimer) with a botched circumcision into living as
a girl (Brenda) from age 17 months - medical studies changed the
names and it became know as the "John/Joan" case. Dr Money declared
when Brenda was age 9 that the gender re-assignment was a complete success.
However, this finding was
undermined when Brenda grew up with a masculine gender
identity anyway, and eventually decided to live as man, choosing the
name David. Summers notes that "the whole idea [was] that
given hormone treatment and the right social environment, you can
determine gender identity. It's not really quite so simple."


 It is important to note that many boy-to-girl
"transsexual's" do not consider themselves to be
transsexual - indeed they often actively dislike being
called such - they just consider themselves to be girls
and in a medical context suffer from Gender Identity
Disorder (GID). The reality is that young transgirls
often associate the word "transsexual" with TV
documentaries featuring strange balding middle-aged men,
married with children, who at the end of the programme
still look, sound and behave like men wearing
wigs, dresses and too much makeup to their very
discriminating eyes and standards. Young
transgirls simply cannot relate themselves with these
examples of transsexuality - their problems are totally
different, and even passing is rarely one of them.
It is important to note that many boy-to-girl
"transsexual's" do not consider themselves to be
transsexual - indeed they often actively dislike being
called such - they just consider themselves to be girls
and in a medical context suffer from Gender Identity
Disorder (GID). The reality is that young transgirls
often associate the word "transsexual" with TV
documentaries featuring strange balding middle-aged men,
married with children, who at the end of the programme
still look, sound and behave like men wearing
wigs, dresses and too much makeup to their very
discriminating eyes and standards. Young
transgirls simply cannot relate themselves with these
examples of transsexuality - their problems are totally
different, and even passing is rarely one of them.











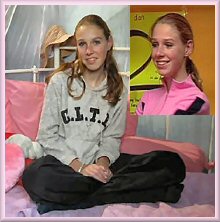
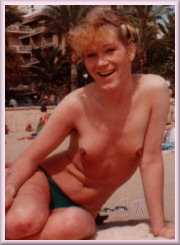
 Ashlyn Parram
(born Lewis) was not allowed to sit an exam at her school because
she was wearing a girl's
uniform. The headmaster only relented after being
shown the Equality Act 2010.
Shown age 11
and 16. (UK)
Ashlyn Parram
(born Lewis) was not allowed to sit an exam at her school because
she was wearing a girl's
uniform. The headmaster only relented after being
shown the Equality Act 2010.
Shown age 11
and 16. (UK)


 There
are two key problems with puberty blockers for a boy to girl:
There
are two key problems with puberty blockers for a boy to girl:



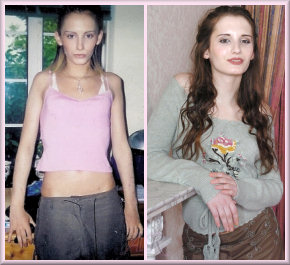

 In her teens (shown age 13/14) Jenny was desperately aware that she was
going through an unwanted male puberty, but it took three and half years on
a waiting list to get a prescription for female hormones. Age 20
(middle) she had an orchiectomy (not GCS) at a local hospital and whilst she
was delighted at the subsequent changes to her body, there were still
obvious problems such as her lack of breast development, a masculine voice,
and facial hair. In 2024, age 21 (right), she became president of the
Students Union at Trinity College Dublin - the premier university in
Ireland.
In her teens (shown age 13/14) Jenny was desperately aware that she was
going through an unwanted male puberty, but it took three and half years on
a waiting list to get a prescription for female hormones. Age 20
(middle) she had an orchiectomy (not GCS) at a local hospital and whilst she
was delighted at the subsequent changes to her body, there were still
obvious problems such as her lack of breast development, a masculine voice,
and facial hair. In 2024, age 21 (right), she became president of the
Students Union at Trinity College Dublin - the premier university in
Ireland. 
 A cartoon
from the 1970's that is still relevant
A cartoon
from the 1970's that is still relevant The Skeleton
The Skeleton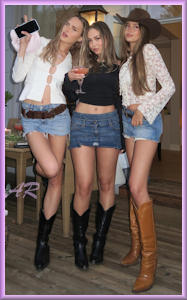

 Back to Articles
Back to Articles (No spaces)
(No spaces)