Breast Development
(In Male-to-Female transsexuals)


Note: I wrote the first version of this page in 1999. At that time, I had read no medical studies describing breast development in male-to-female transsexuals, but the burgeoning World Wide Web had numerous accounts by transwomen (particularly on the GeoCities hosting site) describing their excellent breast development, often after just months on hormones. I took these reports with what I thought was large pinch of salt, but this page was initially far too positive and I began making changes to reduce expectations. Whilst much of the article is now dated, however I believe that it remains a useful read if treated with caution. |
|
For all women, breasts are a very important and very visible aspect of their "womanhood". The all-girl band Pussycat Dolls expressed the feelings of most young girls in their 2008 chart topping song "When I grow up I wanna have boobies".
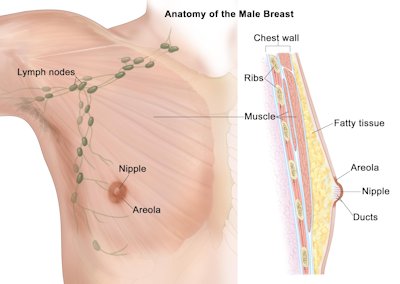
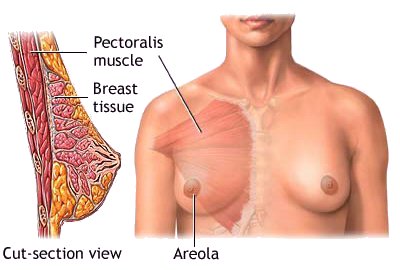
The Breast
Above, the male breast, and below the female breast
Breast
Development in the Genetic Woman Mammogenesis commences at puberty with the onset of oestrogen secretion by the ovaries - usually between the ages of 10 and 12 in a genetic girl. Oestrogen (spelt 'Estrogen' in American English) stimulates breast growth by acting causing enlargement of the mammary fat pad, one of the most oestrogen-sensitive tissues in the human body, as well as lengthening and branching of the mammary ducts. The development occurs according to well-defined milestones called the Tanner stages:
The levels of oestrogen required to cause breast development are surprisingly low - until stage IV the growth of the breast in a girl takes place with oestrogen levels similar to an adult male. That is why about 40% of male children also initiate "Tanner I" type mammary development during their early part of their puberty - their developing testes secrete significant quantities of oestrogens. However, as testosterone secretion also increases the breast development ceases and very few boys reach the Tanner II stage. It takes just two to three years for a girl to achieve the majority of her breast growth. Stage V is aligned with the onset of the menstrual cycle - which results in the production of progesterone for the first time. The presence of progesterone stimulates the partial development of mammary alveoli, so that by the age of 20 the mammary gland in a woman who has not been pregnant consists of a fat pad through which pass 10 to 15 long branching ducts, terminating in grape-like bunches of mammary alveoli. In the absence of pregnancy, the gland maintains this structure until menopause. These ducts are very small and contribute little to breast size - this is a key reason why many doctors consider the prescription of progesterone (associated with pregnancy and lactation) to be unnecessary for transwomen.
Lactogenesis (referred to as the time when the milk "comes in") starts about 40 hours after birth of a baby and is largely complete within five days. When nursing ceases the breast undergoes partial involution, losing most of its milk producing cells and structures. Most woman who have had their first child ultimately end up with slightly smaller breasts than before they became pregnant because they now have less fatty tissue, also once their breasts are no longer swollen with milk they can sag in an increasingly unsightly manner - particularly after multiple children.
Innovolution completes after menopause, when most women move to a smaller bra size. However, since the 1990's hormone replacement therapy has become a very common treatment for women entering their menopause, the renewed influx of estrogen can stimulate breast tissue redevelopment and an increase in bra size.
Breast
Development in the Transsexual Woman
It's important to realise that the results of female hormone treatment eventually become obvious to everyone, whether called breasts or "man boobs". For the pre-transition woman on hormones - it becomes increasingly difficult and embarrassing to go topless - local swimming pool, the beach, or in the bedroom with a partner. It takes about two years
of hormone therapy for a transwoman to achieve maximum breast growth.
Unfortunately, even if this is quite generous, the overall appearance of
the breasts is often hampered by the transgirl having a larger chest
cage than the average cis-woman. Even when their bra-cup
size is actually the same, a transwoman will often consider her bust
development unsatisfactory compared to that of a similarly developed
cis-female. As a result, a majority of transwomen have
augmentation mammoplasty.
In older transwomen, their small breasts are also likely to be
spaced widely, and one breast is often noticeably larger than the other.
These problems make it difficult to monitor the degree of breast
development in mature transsexual women using the Tanner scale.
Similarly, all transsexual women like to 'round up' the breast development
that they
achieve from hormones and other more uncertain methods. But
multiple studies paint a rather depressing picture.
Breast size can be quantified by measuring the maximum
hemi-circumference over the nipple with a flexible tape. The
following table shows the results from one study of breast development,
measured in the sitting position, of 500 transsexual women: It clearly shows that the breasts of male-to-female
transsexual women are considerably smaller than genetic XX women.
To make matters worse, the width of the average transsexual woman's
thorax is greater than that of the average female thorax, and so the
breast development is proportional to the chest size even less than the
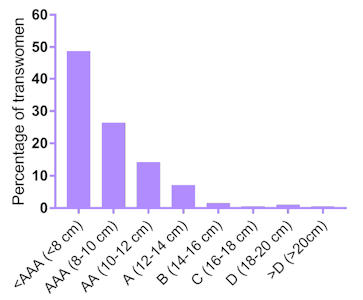
figures indicate. A second study published in 2017 of the breast
development of 229 European transwoman age 18 to 68 (the median
average being a surprisingly young 28) after a year on hormone therapy
(estrogen and anti-androgen) showed similar disappointing results.
The study used the approach of measuring the circumference of the
chest underneath the breasts and at the largest part of the breasts.
The difference between these two measurements was then used to
determine breast growth and
bra size.
The study found: Just 21 (9%) of the women had a bra size of an A cup
or larger (12+ cm difference) 14% had an AA cup (10-12 cm difference) 26% had an AAA cup (8-10 cm difference) 50% had little or no hormone induced breast
development
To compound the disappointment, the study showed
that almost all the breast growth happened during the first six
months of cross hormone therapy (CHT), and that it had tapered to
almost no growth by the final three months. I.e. it seems that
a transwoman has not achieved substantial breast growth after six
months on hormones, she is unlikely to be much better off several
years later. The following chart shows the result of a study that tracked the
breast development of
125 transgender women
(varying in age from 17 to 64) in the months after they began female
confirmation hormone treatment (CHT): The study found dramatic changes in the first 12 months of hormone
treatment, with over 90% of patients reaching at least Tanner III.
But there was only modest improvement thereafter. Although all
patients were judged to have reached at least Tanner III
after 24 months on hormones,
breast development had almost stopped at by this time, and just
8% were Tanner V. After a prolonged pause
breast tissue growth may restart - although there is usually a
trigger such as a change in the hormone regime, an orchiectomy, or SRS. Factors Limiting Breast Development As already noted,
transsexual women generally suffer from limited breast development, with
growth typically stalling at the Tanner III or IV stage. The final amount
of breast development obtained by a transsexual woman from hormone
treatment is very variable and depends on several
factors:
Female Hormones: It
long been known that oestrogen plays the major role in breast tissue
development, with a on-going debate over whether progesterone is also useful.
Growth Hormones: Growth hormones (GH) such as IGF-1
(Insulin-like Growth Factor 1) flood the body of a cis-girl during early
puberty (ages c.10-13). Recent research has found that these
play an important supporting role to oestrogen in stimulating the
development of female secondary sexual characteristics such as breasts.
However GH levels diminish dramatically in late female puberty (c.14-17).
Given that very few transgender girls are prescribed oestrogen hormones
before age 16, this will
handicap their breast developmen. Although IGF-1 drugs can be prescribed, doctors are
reluctant to do this due to the many potentially serious side effects in an
adult. Age: Breast growth is very age dependent. Breast
tissue cells appear to be primed when triggered by hormones to
grow
explosively (mammogenesis)
in the early years of a cis-female puberty, typically between ages 10
and 13. By age 16 this trigger has been disabled. Effects of Testostererone: The body of a transgender
girl or woman has since the foetus stage been
exposed to larger amounts of testosterone hormones than a natal girl.
The cumulative effect on the body is very significant - the most obvious
early differentiation is a penis rather than a vagina, but there does
seem to be a significant impact on potential breast growth as well. Genetics: The lottery of genetics plays a very significant role.
Some people
are genetically predisposed to have copious amounts of fat cells in
therefore large breasts, others practically none. Thus, amply endowed
mother and sisters are a promising sign that development might be good, while flat
chested sisters are a serious worry! Other Factors: There are many factors that come into play in determining the size
of a woman's breasts, including nutrition, exercise, health, and weight.
For example, if a woman's body weight falls below its
optimum then her
breasts can shrink dramatically as the fat cells in them are burnt up
(or in the case of a skinny transwoman are perhaps never deposited),
while if her weight is above optimum then the apparent or relative size
of her breasts may diminish as they are swallowed by the surrounding
"padding".
Age Matters - A Lot Breasts development is very age
dependent.
Empirical evidence strongly suggests that for the best possible
breast development, oestrogen hormone treatment (not
puberty blockers) should begin no later than the first signs of the on-set of male puberty,
typically age 11/12 for most boys, which is a bit older than
girls.
Beginning oestrogen hormone treatment at
this age is likely to achieve breast growth close to that of pubescent
CIS girls.
Relevantly, this has for decades been
the age at which intersex children being raised as a girl are
prescribed elevated estrogen therapy
Since
about 2001 it has become common for young transgirls to be
prescribed anti-androgen 'puberty blockers' at age 11 or 12. These have very
important effects such as preventing facial hair and the voice
deepening. But
they don't seem to stop the biological clock
on cell aging or growth hormomes levels that maximise female
breast development between ages 11 and 15. Thus the potential breast
development
still rapidly falls away to a much lower level than if hormonal
treatment was started well before age 16, ideally by 11 or 12.
After age 18 (the end of puberty for most teenagers) it is impossible
to predict the amount of breast development resulting from beginning to take
female hormones - other than saying that the older you are the more modest
the result is likely to be. Realistically, a 40-year-old can only expect breast budding and a small A
cup, anything more is a bonus.
There seems to be
no medical studies of the effects of hormone therapy on very young
teenage 'XY' girls, possibly because (in Europe at least) this often
involves medically unsupervised self-medication and the results are
unverified. The
Standards of Care Version 7 - published in 2012 - prevents (for many
good reasons) the hormone treatment of adolescents under age 16 and as
result in the early years of this century almost no reputable
medical professional in Europe would prescribe female hormones to a
transgirl under 18.
However, doctors are
ceasing to be dogmatic about following the standards rigidly because of
the self-evident success of early intervention, e.g. in 2016 the UK's
NHS abandoned its minimum age 16 policy for the prescription of hormones
for transgender children.
Transgirls under 16 now have a significant chance of being
prescribed estrogens, rather than just puberty blockers.
Self-Deception
The results of the survey were very confusing. All seven respondents who had begun taking hormones between
16 and 19 were unsatisfied with their hormonal breast development (claiming
only an A or B cup), but none had yet had breast augmentation.
By comparison, a majority of the 39 respondents who started hormones age
20 or later claimed to have achieved very good breast development (C or
D cup) from hormones, however 27 have since had breast augmentation
surgery. I struggled to believe the survey results for the over
20's.
There is undoubtedly a degree of wishful thinking and 'rounding up'
in the breast measurements and bra sizes claimed by transsexual women.
In particular, the claims often made by middle aged transwomen to have
developed large breasts after a year or two on hormone therapy are
improbable and should be treated very sceptically. In many cases I
believe that they have actually had breast augmentation, and in topless photos scars are hidden by using make-up and photo
manipulation.
My conclusion is that most adult transwomen achieve only
Tanner III "A" or small "B" cup breasts from taking estrogen hormones, although a
lucky few will get adequate
- even generous
(a very few!) - breast development.
The Exceptional ...
Television star
Jazz Jennings is a "pin-up girl" for the benefits of early female
hormone treatment. She was on [male] puberty blockers for many
years - probably from age 10 - and was still flat-chested when she
turned age 15. However, she then began taking estrogens and her
breast development thereafter was remarkable. She was initially
reluctant to wear a bra, but by age 17
she was Tanner V and
had grown to a 34D/E cup!
Her
large breasts
forced her to wear a bra for comfort - "I have boobs [and] need
to wear bras". A year later, age 18, she launched her own
Jazz bra.
Even among teenage cis-girls, Jazz's breast development is well above
average, as she acknowledged herself in a YouTube video soon after
turning 17: "I did not get any surgery on my breasts, and surprisingly they
have grown to be the large size that they are today. Anyway, the
reason why my boobs have grown so large is because my mom has really
big boobs and I feel like her genetics is what caused me to ...
blossom like this. I got lucky ... I've been very fortunate to
have my breasts grow the size that they are today and it's something
unexpected. [My] endocrinologist ... said she has never really
seen anyone develop the way I have in terms of my boobs." ... and the More Likely The early prescription of
oestrogen hormones has many benefits for transgirls but guaranteed good
breast development is not one of them. In 2001 I developed a 'rule
of thumb' that a genetically XY transwoman's best possible breast
development from hormones was a bra-cup size less than her XX mother. I
soon discarded this theory in the face of supposed "evidence" that this
was a very pessimistic view, but I have now reverted to my original
supposition. 1970/80's celebrities such
as
Eva Robin's,
Roberta Close and Amanda Lear
who began hormones in their teens never reached more than a B-cup.
Another television star,
Valentijn de Hingh, is perhaps a good example to compare with Jazz as
her life was closely followed by Dutch television from age 8 to 17.
Although born physically male, her parents accepted her desire to be a
girl and she transitioned when nine. The Standards of Care
were then stretched to the limit - she started to take puberty blockers
at 12, female hormones at 16 and had her sex reassignment surgery at 18.
Since then she has been working as a highly rated model, although just outside a Top
100 "super-model" ranking.
The typical adult natal male chest has nipple–areola complexes
(the darker part of the breast around the nipple) that
are far apart, with a paucity of upper pole skin and high, flat
inframammary folds.
The areolae of a man
averages about 25 mm (1 inch) in diameter, but few women are under 30 mm
and 50 mm is common, whilst the areola of women who have large breasts or who
are lactating may be over 100 mm (4 inch) in diameter.
Unfortunately, transsexual women tend to have male type arealoe,
even those lucky enough to otherwise have excellent Tanner IV or even V
breats development. This seems to be a genetic (male XY) limitation. Not only do young
transwomen who start hormone treatment in their teens often suffer from
this problem, but it is also common with AIS women (also genetically XY) whose average breast development exceeds
that of (XX) cis women.
One positive is that because the breasts of transsexual
woman rarely reach full Tanner V size and maturity, their nipples often
remain very prominent - and there are few complaints about this!
After decades of debate a medical concensus has emerged that
progesterone exposure is vital for optimal breast maturation
with areolar growth and size. This is just as relevant for transwomen
as it is for teenage ciswomen.
Hypoplastic
Breasts Low-cost anti-androgen's such as Spironolactone, Androcur or
Finasteride are often taken as part of a transwoman's hormone
regimen. However, there is evidence that excessively high doses of these
(e.g. from self medication) can cause
incomplete breast development. The use of a "cocktail" of hormones that
includes both oestrogen and progesterone may help reduce hypoplasticy,
there is also anecdotal evidence that rubbing a progesterone cream into
the nipple area can help.
Breast Augmentation The overall effect and appearance of their hormone-only induced
breasts is judged unsatisfactory by some 50-60% of MTF transsexual
women, and the vast majority of these seek
augmentation mammaplasty (breast implants).
It should also be expected that the breasts will grow unevenly, e.g., the
right may become much fuller that the left. In the long-term the
differences will mostly even out, but even in mature genetic women there
is often a quite visible difference in size and shape between the left
and right breasts when a study is made of them. But if the
difference is excessive (e.g., a cup size), to the
extent that one breast
has to be padded, then this can be largely eliminated by the use of
different size breast implants. Breast Cancer
Breast tissue means the risk of breast cancer.
Breast cancer is the primary cause of death of about 6% of cis women in
the UK, whilst it's negligible for cis-men. When this article was first written in 1999, breast
cancer was simply not considered relevant for transwomen as so few cases
had been observed. That was
despite the fact that transgender women who take high levels of estrogen
develop breast tissue similar to that of cisgender women, comprising
breast ducts, lobules, and acini. It's now clear that the lack of
cancer cases was due to the small number of transwomen, and the
fact that the vast majority of these only started taking hormones to
develop their breast tissue in their 30's or later.
Breast cancer also has to be added to the list of
potential problems. It increasingly seems that a transwoman who
starts hormone therapy in her teens is as likely to die from breast cancer
as a ciswomen - there hasn't been enough research done to date to say if
the probability is more or less.
All transwomen taking hormones should regularly check their
breasts. Signs of breast cancer include a lump in the
breast, a change in breast shape, dimpling of the skin, fluid
coming from the nipple, a newly inverted nipple, or a red or scaly
patch of skin. Transwomen over 50 who have been on hormones
for ten years or more should have regular mammography screening. One step forward, two steps back During the 2010's I have become increasingly puzzled as to why so
many young (teenage) transgirls
seem to have so little breast development after several years on
hormones. It just doesn't align with the evidence based experience of teenage
trangirls in the 1990's and early 2000's - most reaching at least a B cup.
After consideration of what may have changed, I think it must be the
hormone regimen. Teenage transgirls in the 1970's through to the 1990's often
self-medicated and took relatively high doses (by current standards) of
estrogen hormones - often dubiously purchased without a prescription from off-shore pharmacies. One of the most
popular brands was 'Premarin' - a natural conjugated estrogen extracted
from the urine of a pregnant mare. This is easily assimilated by
the human body and it strongly promotes in a teenager the development of
female secondary sexual characteristics such as breasts, a feminine
pattern of fat distribution, and even (anecdotally) skeletal
characteristics such as a widening of the hips if started early enough. In the early 2000's there was a massive clamp down on off-shore
pharmacies, whilst at the same time the medical profession began treating
transgirls under the age of 18. The prescriptions being given to transgirls
were usually for
anti-androgen puberty blockers such as Lupron (Leuprolide
Acetate) from age 14, with a relatively low dose of a synthetic estrogen
steroid hormone such as estrodial only being added when they turned 18.
Potent estrogens such as Premarin are never prescribed.
The end result of the current approach is a
twenty-something transwoman who despite (or rather, because of) years of medical
treatment still approximates a young teenage boy physically, whilst in the
same time her younger sister has transformed into a buxom woman.
I began taking female hormones
age 29. This quickly resulted in
visually very obvious breast development,
which was embarrassing as a man. I will
never forget a rather tipsy girl in a bar brutally telling me "You need a bra"
- and she was right.
However, the growth soon slowed and had stopped at a 36B cup by the
time I transitioned age 35. Post transition I generally wore
M&S padded bras, and occassionally a push-up bra to show some cleavage. "Are they real" was the obvious if unstated
reaction of my family and old
friends.
Whilst generally happy with them, I
eventually agreed with my boyfriend that my natural breasts were on the small
size and
I had breast augmentation surgery to a D cup.
Although
often only partially developed, the breast structure of a
transsexual "XY" woman is basically the same as a genetically
"XX" woman after the first phase of mammogenesis. Thus,
medical information and rules about female breasts (including
the need for regular breast self-examination and mammogram's)
apply just as much to transsexual women taking oestrogen as they
do to genetic cis women. Assuming that hormones is the
right route, patience is essential, it will take at least two
years to achieve full breast growth and some imperceptible
changes will continue for the rest of your life - as trying on a
very old bra will reveal.
It's undisputable that the earlier in life that oestrogen therapy begins the better
the results will be, although
some girls who began treatment as young as 16 still have
only small Tanner II/III type breasts many years later.
However, as discussed above, I suspect that
current medical treatments are now limiting breast growth in young transwomen.
Transsexual women starting hormone treatment over the age of 18
will be lucky if they eventually genuinely fill a "B cup" bra from
hormone use alone, and those over 30 an "A cup".
If
letters are important it should be remembered that despite a perception
created by television and the press, the average
cup size
of a genetic cis-women in Europe is actually only "C".
Taking hormones hoping to somehow become a closet page 3 girl -
but without anyone at work or even the wife noticing - is simply
unrealistic. Breast growth is irreversible without reduction
surgery, stop taking the hormones and the breast growth that has been
stimulated will still be around ten years later, it does not melt away.
Examples
Please contact me if you have any comments.
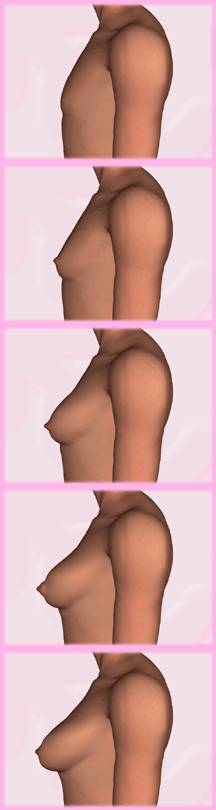
Above.
A transwoman who began taking estrogen age 30. Her breast
development is shown after 0, 12, 19 and 28 months. She has reached
a good Tanner III, but little further breast growth is likely. Below.
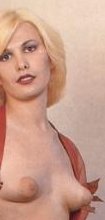
A 24-year old transwoman
after 30 months on estrogen hormone therapy. Her Tanner III
breast development is typical for her age, but she was disappointed
and later had breast augmentation.
Below. Jessica
began hormone treatment age 20 and documented her breast
development over the next four years, which has resulted in
good Tanner V development.
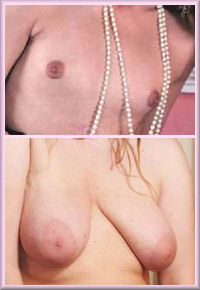
Below. Photos of transwoman collected from public domain sources.
Below. Photos sent to me by transgender women of their
breast development. I can't vouch for their accuracy.
|
 The display or even the indication of breasts is
instinctively viewed by observers as strong evidence that someone is
female. Breasts are
regarded by both men and women as a key aspect of
The display or even the indication of breasts is
instinctively viewed by observers as strong evidence that someone is
female. Breasts are
regarded by both men and women as a key aspect of  The
development of breasts gives the male-to-female transgender woman a
tremendous confidence boost, and powerfully identifies her as a female
to others. It is also impossible to ignore that the fact that
breasts are immensely strong sexual symbols, and secondary sexual organs
whose presence can be enjoyed by both the owner and their partner.
Unlike a vagina, breasts can be easily and acceptably be publicly
displayed in either part (cleavage) or full (e.g. topless sunbathing),
or prominently implied underneath a skimpy top. Bra's and
often breast forms/padding are essential early
The
development of breasts gives the male-to-female transgender woman a
tremendous confidence boost, and powerfully identifies her as a female
to others. It is also impossible to ignore that the fact that
breasts are immensely strong sexual symbols, and secondary sexual organs
whose presence can be enjoyed by both the owner and their partner.
Unlike a vagina, breasts can be easily and acceptably be publicly
displayed in either part (cleavage) or full (e.g. topless sunbathing),
or prominently implied underneath a skimpy top. Bra's and
often breast forms/padding are essential early Whilst
a majority of transsexual women eventually have
Whilst
a majority of transsexual women eventually have 





































 The result is a very effective prevention of physical masculinisation
such as facial hair, deepening voice and muscle build up. However, the medications do
nothing to promote feminisation and breast growth
(indeed they may hinder this), with estrogen being added very late in
the puberty phase, and of
a type that breast tissue is not sensitive to.
The result is a very effective prevention of physical masculinisation
such as facial hair, deepening voice and muscle build up. However, the medications do
nothing to promote feminisation and breast growth
(indeed they may hinder this), with estrogen being added very late in
the puberty phase, and of
a type that breast tissue is not sensitive to.





































 Back to Articles/em>
Back to Articles/em>Last updated: 22 June 2018
|
Formerly the "Birth of Venus"
(c) 2000-2025 Annie Richards |
 (No spaces)
(No spaces)