
(Part 2)
|
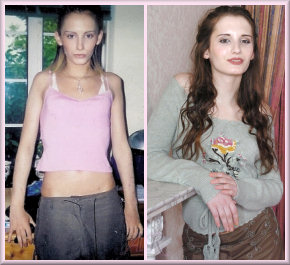
Recent years have seen a vocal campaign against what are seen to be 'privileged' groups - with middle-aged white Caucasian men the most targeted. However, the 2016 film White Woman highlights how a woman can manipulate her way through life if she is white, pretty and young. A transitioned western MTF transgirl arguably also has many potential privileges and advantages:
The "Age 16 Passability Advantage" Whilst the exact age can vary slightly, there does some to be huge divide in the ability of transgirls who began oestrogen treatment by age 16 to pass as female, compared to transwomen who started age 17 or later. The following table compares the effects of beginning female hormone treatment before a male puberty starts (which is typically age 12), with beginning treatment after male puberty has completed (i.e. after about age 17). Extensive experience with intersex but "XY" female individuals indicates that for the very best results, low-level oestrogen treatment should be started at age 9, and stepped up to "puberty" levels at 12. Commencing treatment during puberty will produce mixed results between the two poles - e.g. the voice may have already deepened irreversibly but facial hair growth is prevented or greatly reduced.
It's become certain that the early use of hormones helps to restrict height. Estrogen accelerates the completion of growth in the growth plates (the zones of growing cartilage near the ends of children’s bones) in girls, thus reducing their average adult height compared to men. One young transwoman blames her short 5ft 2in stature - compared to her 6ft plus brothers - to excessive HRT too early. It's less clear how much impact early hormone treatment has on skeletal characteristics such as foot size and pelvic width. For example pre-puberty, the pelvis of boys and girls are indistinguishable, but post-puberty the female pelvis widens substantially. This change is thought to be caused by estrogen, and studies of FTM transboy's shows that hormone treatment suppressing estrogen and raising testosterone treatment can prevent this differentiation in transboys. Oddly, there are no studies showing that conversely young transgirls taking estrogen, plus anti-androgens to suppress their testosterone levels, are likely to develop a wide, female-type pelvis. Whilst this seems likely, the evidence is just anecdotal and medical studies are needed to prove significant skeletal changes rather than just fat redistribution.
Hormone Regimen's for Transsexual Girls From studies of patients with Turner syndrome it has been suggested that to ensure normal pubertal growth, physiologic oestrogen replacement should be started at the appropriate bone age of about 11 years and should not be delayed in the hope of achieving a greater mature height. Batch et al suggest a regime of 5 micrograms of ethinyloestradiol daily for the first 6 months, increasing to 20 micrograms daily by the end of puberty.
Soule et al. suggest that the best course of action
may be to perform a orchiectomy just before puberty (at 11 years in a case
quoted) followed by oestrogen therapy (ethinyloestradiol 2 micrograms daily,
gradually increasing to 20 micrograms over 2 years, in the case quoted) with
regular bone density measurements. This policy, it is suggested, reduces any
slight risk of malignant transformation of the gonads and ensures adequate
oestrogen activity throughout the critical years of bone accretion. However, oestrogen levels are higher in XX girls than in XY
boys, even in childhood. XX girls start producing oestrogen at 8 or 9
(i.e. a year or two before breast development) so several clinicians
therefore recommend early oestrogen supplements in XY girls, irrespective of
whether or not the gonads are in place. Dr. Stanhope suggests 1
microgram ethinyloestradiol per day from age 8-9, with an increase at about
11-12 years. Females Hormones and Attractiveness A very awkward problem for psychologists advocating delayed hormonal treatment for young transgirls is that as result they will be physically less attractive as a woman to men. There is a strong and direct correlation between a girl's oestrogen levels during puberty and how attractive and feminine she is perceived as a woman. For example, the hormone has lasting effects on bone growth and tissue formation as well as the skin’s appearance during the average seven-year-long puberty. Miriam Law Smith of the University of St Andrews states the hormone has a hormone has a crucial role in determining facial appearance, giving 13-year-olds doses of oestrogen will "certainly may make them more attractive [to men]" although she adds "who knows what other effects the hormone may have?" As regards the last comment, pubertal girls who have been prescribed oestrogen to prevent excessive height (over 6 feet) may according to one study subsequently suffer from lower fertility.
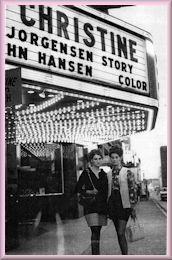
Since the 1960's the medical professional has been puzzled why one child may determinedly transgender, whilst his/her brothers and sisters are equally determinedly cis-gender. If as some leading medical practitioners were suggesting (most notably Dr John Money) external factors during childhood played a critical role in determining gender, it seemed reasonable to predict that if one child is transgender, there was a good probability that their siblings were as well. The theory got some support when in 1970 two American half-sisters - Lauraine and Lenette - were outed as having been born Cary and Burt. They transitioned together and Lorraine had SRS age 26, the younger Lenette had to wait another six months as the clinic refused to perform her surgery until she was 21. They not only appeared in newspaper stories at the time, but were mentioned in many medical textbooks published the 1970's.
In 1993 French newspapers briefly covered the story of supposedly transgender sisters Dominique and Alix, born brothers Patrick and Yannick. Patrick had shocked his parents by announcing on his 18th birthday that she was a girl and wanted to be called Dominique, and allegedly had SRS. A few years later her younger brother Yannick made a similar announcement and asked to now be called Alix. But the newspapers fed the story were unable to obtain a picture that showed Alix as anything other than a rather effeminate looking 18-19 year old teenage boy. Also, Alix's claimed boyfriend turned out to be a divorced 41 year-old who had two sons of similar age to Alix. It all seemed decidedly dubious and the newspapers soon gave up on the story.
In 1996 an American television talk show featured exceptionally close sisters who did everything together. Two 20-something sisters, Mi and Ana, were planted in the audience, and it was eventually revealed that they had been born brothers and were male-to-female transsexuals. In the 21st century the transgender population has soared, and perhaps inevitably there has a emerged in to the public domain a few instances of two brothers becoming sisters. For example, in February 2016, a 23 year-old barmaid working at The George pub in Cork - Jamie O’Herlihy - came out via a YouTube video as being transgender. For several years she had worked as a drag queen at a gay bar but had transitioned to female and begun taking female hormones the previous November - retaining her androgynous first name. The news attracted only mild interest until Closer magazine discovered that Jamie's younger 20-year old sister Chloe had been born Daniel. After a difficult final year at school as a boy, Chloe had quietly transitioned to female in the summer of 2015, before starting a college course to train as a hairdresser. The story of the two transgender Irish sisters went viral, and they appeared in newspapers around the world, as well as on Irish television programmes such as This Morning and the Ray Darcy Show - often accompanied by their mother Sarah. The money earned hopefully helped to pay for Jamie's facial feminisation surgery, and Chloe's SRS in 2019. Almost simultaneously, another story concerning two American transgender sisters was unfolding. In 2016 14-year old Matthew Whitley transitioned and became Madelyn ("Maddie") Whitley. Her twin brother followed just a few months later, transitioning as Margo in January 2017. Both Madelyn and Margo have since been signed by model agencies and now work with great success as female models.
On 11 and 12 February 2020 the 23 year old sisters received surgeries to affirm their gender identity. Dr. Jose Carlos Martins of the Transgender Center Brazil performed five-hour surgeries on the sisters one day apart. “This is the only reported case in the world of twins who were presumed to be male at birth undergoing female gender confirmation surgery together” the doctor claimed. The global transgender community now numbers in the millions - compared to hundreds in the 1950's, thousands in the 1960's, and tens of thousands in the 1970's. If the theories of Dr John Money et al are correct then there should now be a very large population of transgender siblings. But there aren't, so their theories are incorrect. Unfortunately this doesn't help us understand a situation where in the UK the ratio of children with gender identity disorders has in just two decades changed from 1 in 10,000's, to 1 in 100.
Passing and Sexual Orientation There seem to have been no formal clinical studies, but it seems certain that young male-to-female women are far more likely to complete their transition and settle well into their new lives than those who transition at a later age. About 95% of natal "XX" women consider themselves as being heterosexual. In comparison, studies of the sexual orientation of post-SRS transsexual women indicate that only half are heterosexual and exclusively select males as sexual partners; nearly one-fifth are lesbian and sexually attracted only to females; and about one-third are bisexual. However these studies cover all age groups (with an average age in the 30's or even 40's), and are almost certainly not representative of the relatively few young transsexuals who transition before the completion their male puberty. It is very likely that when compared to older transwomen, a far higher percentage of young transsexual women identify themselves as heterosexual and attracted to men. Indeed, for under 21's, I would suggest that there are very few girls who do not consider themselves to be heterosexual, and have or would like to have, a boyfriend.
Unlike older transsexual women, young transsexual girls rarely have had any sexual activity before they transition, and if they do it's likely to be of a homosexual nature, generally playing a female role during intercourse. Mentally they are often only erotically stimulated by men, although overall their sexual urges may be very low because of puberty suppressants. When released from such drugs and placed on hormone therapy, they become just as interested in boys and men and sex as other girls of their age - if not more so. "G", a nearly 16-year old transgirl undergoing an intense female puberty thanks to being on hormones illicitly obtained by her parents, may be quite typical when she writes: "I can't stop thinking about my [neo-vagina] ... I want to be ['screwed'] by any guy in sight. I was even thinking about my teachers and my best friend's dad." But this girl does not expect to undergo SRS for years yet.
Hopefully G will be able to emulate Veronique Renard, who has happily led a very active love life as a woman since her teens. She may have the youngest patient in Europe when she had SRS in 1984, but the resulting advantage was immense:
Unlike older transsexual women - young transsexual girls rarely have any problems passing easily and naturally as female, readily assimilate themselves as women. For example, in one survey (Sex Reassignment of Adolescent Transsexuals: A Follow-up Study, Cohen, 1997) of young transsexuals, all the male-to-females were satisfied with their appearance after hormone therapy, and it was the interviewer's observation that it was difficult to discern any signs of their [genetic] sex. Most of the girls had been approached in a flirtatious manner, and not one had been approached by strangers as if they were still of the male sex, 60% expressed satisfaction with their vaginoplasty, and had experienced sexual intercourse without problems. The author of the study suggested that part of the adolescents' success was due to the fact that they more easily pass in the desired gender role because of their convincing appearance. With one exception the voices of the girls were not male sounding, and early anti-androgen treatment apparently had acted in a timely way to block facial hair growth and the lowering of the voice.
Nevertheless, success in passing may well be an important factor in young trans-girls being far more likely to have a heterosexual sexual orientation than transsexuals who transition as adults. It's clear that trans-women who transition at a young age are almost always physically able to go stealth, they typically do as soon as possible, and often quickly begin to have boyfriends and eventually a husband. The desire for a normal relationship with a man tends to pull the stealth transwoman away from any open acknowledgement of her transsexuality and male past, she believes (unfortunately often correctly) that the relationship may not survive this becoming known to him. In the balance between personal happiness and revealing "the whole truth and nothing but the truth", most people choose happiness. Based on anecdotal experience, when a young transwoman out's herself, most (but not all) soon regret.
Sex Re-assignment Surgery After hormones and transition, the next and final step is sex-reassignment surgery. Extra-ordinarily, only about 1% of SRS operations performed by western surgeons are on girls under age 20 (almost all of whom are 18 or 19). The reasons seem to be a combination of the Standards of Care guidelines, the need for a two year real life test when a hormone supported transition can only begin no earlier than age 16, money, the requirement for parental
By interesting contrast, one study of 195 Thai male-to-female transsexuals found that "many participants had transitioned very early in life, beginning to feel different to other males, and identifying as non-male by middle childhood. By adolescence many were living a transgendered life. Many took hormones, beginning to do so by a mean age of 16.3 years, and several from as early as 10 years. Many underwent surgeries of various kinds, on average in the twenties, with one undergoing SRS as early as 15 years".
Another extraordinary tale of determination is Lucille. Born in 1986 as Lucien, he knew even at pre-school that he was a girl, not a boy. By secondary school his long hair and wearing of girl’s cloths led to teasing and worst. He sought medical help but faced three year waiting lists. After leaving school he obtained a job as a female hairdresser but lost it after being out'ed. In desperation he persuaded a private medical clinic that he was from a noble family and had well-to-do parents. In June 2006 - age 20 – the clinic performed sex reassignment surgery and breast augmentation on her.
If a transgirl has been determined in her identification as female from a very young age, then (as described above) there are many advantages in the prescription of puberty blockers and even female hormones by age 12. One advantage would seem to be that the penis remains tiny (maybe an inch in length) and the testicles do not drop. But this suppression of developing a male body actually creates a serious problem as most SRS procedures use scrotal and penile skin to create the neo-vagina, and there may be simply not enough skin to do this. A high-profile example of this is the experience of American TV reality star Jazz Jennings, who grew up as a girl from age 5. Age 11 she began taking puberty blockers and age 14 she began to take estrogen. The results were textbook - her body developing as female rather male as she moved through puberty, including very generous breast development. Meanwhile her penis shrunk to almost nothing, and her scrotum didn't drop. But when she sought GCS age 17, her doctors found that there wasn't enough penile and scrotal tissue to reconstruct her genitalia using the standard penile inversion technique, or any variant of this. Jazz said in a video posted on her YouTube channel: "I didn't have growth in that region and because there was a lack of tissue, they didn't have enough material to construct the vagina. So they're using a special procedure where they extract my peritoneum lining through my belly button and they use that and they harvest it and they use it to create a vaginal canal." Dr Marci Bowers eventually performed the procedure, but as feared it did not go well and Jazz had serious complications. Her shallow neo-vagina split open just a week later when attempting to dilate, which required an emergency surgical procedure. Later her vagina was relined using skin grafts from her calfs. This surgery went quite well, but yet another corrective procedure was still required to improve the external appearance of her clitoris and vulva area.
Maxim Magnus had very similar problems to those experienced by Jazz. She began female hormones at age 14 and had SRS in 2016 when age 18, but soon encountered major complications:
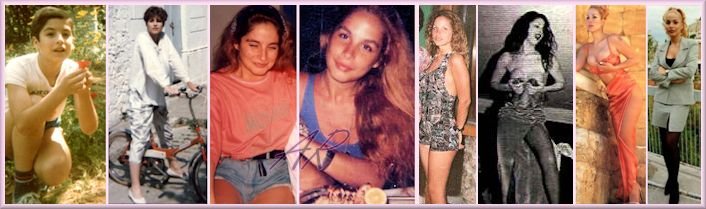
She had recently been discovered as a model and was being hailed by the likes of Vogue as "Fashions next big star". Instead she was forced to retire from modelling for a year. In 2019 she posted "I’m about to have my fifth surgery in two and a half years to correct more issues related to my SRS [but] in spite of everything, I’m glad that I had SRS" [Note: Articles and interviews about Maxim give her confusingly different ages, but the consensus seems to be that she was born on 15 April 1998.] Victoria Bazúa In 2024, the very young Mexican actress Victoria Bazúa (born 29 June 2008 as Victor) shot to fame after appearing in the Apple TV+ series Land of Women. With her attractive looks, slight frame (55 kg), modest but very leggy 5' 7" (170 cm) height (an inch more than when she tested for the role!), fun dress style and boyant personality she was a clear standout. In the first episode it is revealed that her character, Katie, was a lesbian, in the second - to the shock of many viewers - we discover that she is also a transgirl. In pre-release marketing the producers had revealed that Victoria was herself actually trans. In a subsequent interview Victoria says “When I expressed to my parents that I wanted to transition, that that’s who I was, I think I was two years old. I was like, ‘Mommy, I’m a girl.’" She was then always called Victoria and has no memory of her male name. By seven she had been totally accepted by her family as a girl, and she went to school wearing a girls uniform. When "the whole process of ... estrogen and hormones happened around 12, before puberty. I never really went through male puberty, I guess.” Victoria is often referred to as being post-GCS, but is silent about this - possibly because she had the procedure years before the legal minimum age of 18 that applies in many countries. Age 14 she was taken on by modelling agencies began working as a female model - initially for the locally based Queta Rojas, but the multi-national agency Paragon moved in when her potential became evident. She also started taking acting classes and age 15 - still physically growing as she completed her estrogen induced female puberty - she auditioned for the role of Katie, her first acting job. The producers had expected to fill the part with a twenty-something cis-woman actress who was convincing as a younger transwoman - but instead Victoria appeared from no where and was a perfect fit.
From the left, Victoria Bazua age 14 (in a photo booth), 15 (modeling), 16 (in Land of Women), and then photos of her age 17 or 18.
In interviews, Victoria Bazúa constantly emphasis the importance of her family (and in particular her mother) during her journey from a baby boy to a teenage girl: "My family has supported me all along. It hasn’t been easy, and there have definitely been some obstacles and rocky situations. But family support is the most important and valuable thing you have. Having a support system is what got me here. That’s the key."
Clearly a positive
reaction from their parents when a child comes out as out as trans is a
huge support and the impact can’t be underestimated. A supportive
family can make huge difference to a transperson’s mental well-being in
the long-term, and their relationship with the rest of the family will
be much more positive, in particular with the parents. One supportive
mother of a young transgirl said:
The active support of their parents is also essential for transgirls when trying to find help at school or from the health system. Considering all the advantages of the early treatment of the young transgender children, it's unsurprising that this is now increasingly demanded by knowledgeable parents increasingly informed via the Internet.
Parents are undoubtedly influencing a 'system' and medical profession that was in the 1990's retreating rapidly from early treatment and accommodation of young transsexuals. After a decade long reaction to the tragic David Reimer affair, it has become recognised that it is necessary to separate and differentiate between the voluntary and non-voluntary gender reassignment of children. While numbers are still small, there is nevertheless an increasingly willingness by doctors and the "system" to support and aid the early reassignment of children. The revised guidelines in the current version 6 of the "Standards of Care" issued in 2001 makes it slightly easier for young transsexuals to officially obtain treatment - including puberty-delaying drugs but not female hormone therapy for those reaching their teens. But doctors still face circumstances where a failure to support young transsexuals in order to comply with guidelines can seem at best totally unreasonable. For example, in 2006 a 5-year boy was allowed to enrol in kindergarten as a girl with a "gender-neutral name" in Florida, USA, having been diagnosed with gender identity dysphoria (GID) two years ago earlier. The parents said the child refused to wear boy's clothing and repeatedly said she hated having a penis - often trying to hide it between her legs. Officials said that were already a number of trans-students in the school system but none as young as kindergarten age, they expected that the youngster would go unnoticed as a girl. Can she be denied female hormones at age 11-12? Meanwhile, in Japan a 7 year old boy with GID, Ryoko Kanda, has been allowed to enrol as a girl at a school is in the prefecture of Hyogo, about 270 miles west of Tokyo after being diagnosed with gender identity disorder at age 6. The school has not told other parents about the switch, and a spokesman for the local school board said there had not been any complaints from other students or from the boy's parents since his enrolment. He stated that the boy's name is listed with girl students, she uses the girls' bathroom, attends a girls' gym class and wears a girl's swimsuit at the school pool. The official also said "At this point, we are relieved that the child was accepted into [second] grade and is being raised in a healthy manner", he added that the school district would watch his case closely and reassess the decision as the boy reaches puberty. Katsuki Harima, a psychiatrist specializing in gender identity disorder at Tokyo Musashino Hospital, said the decision to allow the boy to enrol as a girl seemed appropriate, but would get complicated as he grew older. Harima said the boy is not old enough to determine whether he really has the disorder. A boy who behaves like a girl does not necessarily have gender identity disorder and he could discover as he grows older that he wants to be male. Although identified at birth as boy, Norwegian Siri Lehland always wanted to wear girls cloths and by age 10 she was adamant that she was female. Her mother, Katja says:
With the strong support of her mother, Siri transitioned by age 12 and began to aspire to be a model. Four years later she appeared on the front cover of the Norwegian edition of Elle magazine in 2018, still just 17, much to the delight of her proud mum! Progress since 2001 This article was first written in 2001, revisiting it a decade later there has been some progress in the treatment of young transsexuals. There can be almost no doubt that a series of highly publicised transgender success stories - basically young boy-to-girls who thanks substantially to early medical treatment look and sound like teenage girls - have helped this immensely. Another generally very positive development has been the appearance on social media such as YouTube, Facebook, Instagram and Twitter of openly transgender girls who then act as an inspiration and source of information for other girls
Overall, huge progress has undoubtedly been made since 2000 in the treatment of transgender children. Further the increasingly positive image presented about gender dysphasia in social media, in television programmes such as I am Jazz, Transparent and films such as the Danish Girl has resulted in young children identifying themselves as being transgender in unprecedented numbers. In the USA and Europe the number of under-18 children reported as having gender identity disorder has doubled annually since about 2010. As the same time, the number of girl-to-boy has increase from about 25% to over 60% at some clinics. Little by little an increasing number of clinics are now willing to help young transsexuals with medication and even surgery at an early age. Two examples:
USA: In 2007 the pediatric endocrinologist at the Children's Hospital Boston, Dr. Norman Spack, set up a clinic for pre-adolescent transgender children. Dr Spack uses drugs to delay the first stirrings of a youngsters' puberty, typically age 12 to 14 for a boy. The effects of these puberty-blocking drugs are reversible but is not the case with hormones. Dr Spack is flexible about the age he prescribes estrogen - i.e. he's not rigid that the child has to be age 16+, but will only do so after months of consultation with the patient and her parents. He says "When kids take this step, they are rewriting their own future: The hormones have a powerful, pervasive effect, changing their height, breast development, and the pitch of their voices ... You have to explain to the patients that if they go ahead, they may not be able to have children. When you're talking to a 12-year-old, that's a heavy-duty conversation".
UK: The Portman and Tavistock Clinic in North London was established in 1994 with a particular mission to provide treatment to transgender children and adolescents under the age of 18. It was deemed controversial due to the patients' ages - with critics arguing that the youngsters lacked the ability to consent to the therapies. However Dr Polly Carmichael, director of the service, said it was "better for children not to have gone through puberty before transitioning". But she added: "You are asking someone aged as young as 11 to make big decisions about their adult life and identity. We have to be very careful to keep options open".
Below is table from the Trust which provides a detailed breakdown for referrals age 17 and over.
Three standouts from the table are:
In 2020 there were media reports that the clinic was over-whelmed and was prescribing life-changing hormone treatment and even surgery to children without adequate rigour, often after just one short consultation. After numerous serious complaints were upheld, the clinic was closed in July 2022. Whilst this was probably justified, it has left the UK with no specialist facility for the treatment of transgender children.
The TV series Germany's Next Top Model (GNTM) has since season 12 (2017) included at least one transwoman contestant every year, all apparently transitioned as a teenager and were post-GCS in their early twenties when the show was filmed. Examples include from the left, Giuliana Radermacher (2017), Melina Budde (2017), Tatjana Quinn (2019), Lucy Hellenbrecht (2020), Alex-Mariah Peter (the 2021 winner), Mirella Janev (2023) and Lisa Del Piero (2025). The programme shows both the advantages that young transwomen have (e.g. height, long legs, a "clothes horse" figure that fastion designers love), but also the disadvantages (voice, close up facials, slight hips and buttocks, appearance in a bikini) that they face as a woman without further extensive feminisation surgery. Their relationship the other models and even the judges was also sometimes complicated due to them being trans.
Perhaps a sign of the progress that has been made in recent years in the United Kingdom are the stories of Campbell Kenneford and Maxine Heron. Maxine Heron was born a born 1996, but she “always knew that I was a girl". She came out age six to her mum when she refused to have her hair cut. "I think it came as no surprise because as soon as I could start to express myself I would always do so in a way that was really female ... I just was always kind of her daughter". Her parents accepted her choice and with their support she had the courage to transition full time when she went to a College of Higher Education, age 16.
After she left college she had a variety of jobs, from receptionist to booking agent. After having SRS (perhaps age 19) she began to work as model. She was completely passable with a very feminine voice, an acceptable height of 171cm / 5´7" and slight weight 63 kg / 138 lbs, but in late 2018 she "decided to come out on social media and tell everybody about my history". The response was very positive, e.g. one photographer who had booked her a few months earlier posted:
The series was shown in August 2019, in episode four Maxine unexpectedly stood up during a meal and revealed that she is transgender to her apparently genuinely shocked table mates.
Ethan was calling himself a girl by age three, and transitioned age nine. She began taking puberty blockers age 10 and estrogen hormones age 13. Evie regularly posts on social media.
Kim Petras A rare example of the medical community responding to the needs of young transsexual may have achieved in Germany when it was revealed in 2007 that doctors had prescribed puberty blocking and later female hormones to a 12-year-old 'Kim', formerly Tim. At age two, Tim was trying on his older sister's clothes, playing with Barbie dolls and saying "I'm a girl." By age four Tim was refusing to get to his hair cut and wanted to cut off his "thing", for the sake of a normal life his parents increasingly accepted their son Tim as being their daughter Kim.
The situation reached a crisis when age 11 Kim grew increasingly distressed at the prospect of becoming like other adult transsexuals "with big hands and deep voices", whom she thought looked ridiculous when they dressed like women. Her father said "We saw Kim as a girl ... not as a problem. ... [she] reacted badly to the first signs of puberty... At that stage we realised that she was terrified of growing facial hair and her voice breaking". Kim’s parents decided to help her get a sex change and consulted psychiatrists across Germany. Some condemned their support of their child’s desire to undergo a sex change and even suggested that she be kept under observation in a closed psychiatric ward. But Dr Bern Meyenburg, the head of a clinic for children and adolescents with identity disturbances at Frankfurt University, concluded that the child was serious. He wrote in his diagnosis: "Kim is a mentally well-developed child who appears happy and balanced. ‘There is no doubt of the determined wish, which was already detectable since early childhood. It would have been very wrong to let Kim grow up to be a man." Dr Meyenburg had once strongly opposed hormone treatment for children but changed his mind when one of his patients refused to listen and ordered hormones over the internet, then went abroad at 17 and had a sex change operation for a few thousand euros. Dr Meyenburg admits that he was angry at the time, but said that today the woman is a law student and one of his happiest patients. He now allows young patients to enter hormone treatment early, before puberty complicates a sex change. "They simply suffer less," he said, "it would have been a crime to let Kim grow up as a man".
Dr Achim Wuesthof, who for many years treated Kim at his clinic in Hamburg, said: "Imagine a man who suddenly starts growing breasts or a woman who starts growing a beard against their will – that is how Kim and people like her experience puberty." Kim was thus prescribed female hormone therapy when just 12, and by age 14 was fully transitioned and living as a girl - with her identity and medical insurance cards changed to her new name and female sex. German law only permits sex-assignment surgery (SRS) at age 18, but Kim apparently had this in November 2008 - just two months after her 16th birthday. This created headlines around the world that proclaimed her to be the youngest person to ever have had SRS, although that claim is false - even excluding XY intersex children. Just two examples are the sad case of David Reimer (age 22 months), and Victoria Beltran whose parents managed to get her surgery when just 15. Also, hundreds of SRS procedures are performed every year on under-18's in Asia and South America, and it seems very likely that some are under 16. Kim handled the intense media interests surrounding her surgery with great honesty and confidence, for example she told one interviewer "I was asked if I feel like a woman now - but the truth is I have always felt like a woman - I just ended up in the wrong body." Since age 18, Kim has concentrated on developing her a career as a singer, with considerable success.
A
Warning In 2018 the British media reported that one school had 19 children (2% of its roll) listed as transgender. Subsequent reports claimed that about 1% of all school children were now identifying themselves as transgender. These percentages were plausible given that about 40 times more children were being treated by the NHS for gender identity disorder (GID) than a decade earlier, the Portman and Tavistock Clinic (mentioned above) had 2,590 children referred to it in 2018, compared with just 77 in 2008. It seems that for good or bad a critical point has been reached where children (particularly in their early teens) are beginning to consciously choose their gender. It is attention gaining and potentially even trendy for a 12-14 year old to proclaim that they are androgynous, transgender, non-binary, etc., with children encouraging each other to transition and request medical treatment such as puberty blockers (available on NHS from age 11 since 2011) and hormones (available from age 16, but increasingly prescribed at 15).
Despite the diverse results of studies, its VERY important to note that many
children who test their gender identify at a young age (3 - 10) will
actually revert to their physical sex by puberty - VERY great care thus
needs to be exercised by both parents and medical professionals to avoid
irreversible decisions and medical actions at too young an age.
Although the incidence of GID referrals
in young children below age 12 is exploding in number, the percentage
that eventually have sex-reassignment surgery is actually declining - down
to just 10% in the UK in 2015.
Conversely, children who begin questioning their gender at an older age seem far less likely to change their mind. As puberty begins. it seems that almost every child who age 12+ begins blockers or hormones will eventually have surgery, and nearly zero later regrets. For example, Jack Green started to show signs of GID as young as 3. By age 9 his mother Susie was letting him dress as Jackie but by age 13 she was veryoncerned about both the resulting bulling and the onset of male puberty. Puberty blockers were obtained from an American clinic and Jackie also referred to the Tavistock Clinic. When it became clear that Jackie was unlikely to have surgery via the NHS for many years due to the long waiting list, Jackie's parents for arranged for her gender confirmation surgery to be performed in Thailand on her 16th birthday. Her mother later saying: "Medical intervention is very important, especially for teenagers who are already in puberty. It's absolutely vital. [Particularly] if you’ve got a child who's suicidal and self-harming because their body is changing against their will,"
Susie's high-profile campaigning for the medical treatment of children suffering from GID extraordinarily led in 2019 to a journalist reporting her to the police for having "castrated her child". No legal proceedings resulted.
As a result, UK guidelines have been revised and in practrice it has become impossible to have SRS in the UK if under 18. The small number of operations (35) previously performed will now happen outside the UK, predominantly in Thailand - were a far larger number already go.
The NHS’s statistics show that the rate of regret around gender affirmation surgeries is very low but apparently a small number of young patients do subsequently de-transitioned as an adult, and they then bitterly regretted having had irreversible 'bottom surgery' as a child. [I have been unable to find even one quotable example of this] As a result, in April 2020 the UK government announced plans to ban all gender confirmation surgery on under 18's. Dr Jane Hamlin, President of the Beaumont Society, a transgender support group, generally supported the decision, stating:
It's difficult to over-exaggerate just how great the advantages of early medical treatment are for the pubescent transgender girl whose body will otherwise rapidly turn in to that of a man, and how much of a disaster each month of delay is. The end of puberty is a fundamental and irreversible physical marker, from which the plausible effects of feminizing hormonal treatments on the body of a transgirl/woman decline with depressingly rapid speed. For any transsexual woman starting treatment when already physically mature (and this merely means age 20 onwards), a muscular and robust stature; a deep and masculine sounding voice; obvious facial beard growth; and a receding hairline, are just four of the immediate challenges that may seriously threaten her ability to pass convincingly as a woman. She also faces the high cost of electrolysis, breast augmentation, facial feminisation, and other risky procedures such as voice feminisation surgery that could have been avoided There is no longer any debate that for the best possible final outcome, the medical treatment of a male-to-female boy/girl with GID should be started as early as possible - ideally before puberty. Decades of slowly accumulated empirical evidence seems to indicate that age 12 or 13 (depending on the individual) is the optimum age for a successfully transitioned transgirl to commence high dose hormonal treatment.
Puberty blockers are a poor second choice, but still far better than nothing. When compared with the experiences of older transsexuals, the results of early hormonal treatment are dramatically positive. It is however important that the girl has already successfully transitioned - this is a key point at which some young boys realise that are making a terrible mistake. Gender Clinics are reporting a near 100% success rate for children who transition, begin hormones and have SRS surgery in the age 16-18 window. Almost all successfully these teenage transgirls identify totally with their female gender and appearance, passing well both psychologically, socially and physically; they are far happier as a female and have no regrets. They still face long term problems as being infertile as a woman, and how to tell this to a fiancée ... but these are a totally different set of problems from that which delaying medical treatment would have imposed upon her - such as an inability to pass due her beard, deep voice, and bald patch.
It is unfortunate that the medical profession is advancing so very slowly, partially due to a lack of facilities and specialists. In the UK the NHS's only Gender Identity Clinic, the Portman and Tavistock Clinic in London, was closed in 2023. This has left a population of over 60 million people with no specialist psychiatric and endocrinology services for transsexual children. There is a valid argument that if medical treatment was not provided to transgirls, some would successfully revert to a male gender. But it equally seems that many would resort to extreme measures, even suicide.
Finally, we appear to be heading to a world where a
substantial proportion of the population will live most of their life in
a gender that does not align to their genetic sex. In the UK less
than 1 in 10,000 children under age 18 were identified as transgender in
2000, twenty year later we seem to be in the situation where about 1 in
a 100 children consider themselves as being transgender, increasing to 3
in 100 if we include those who identify as asexual, pansexual or gender
fluid. This has huge implications in terms of reproduction, and the normalisation families where one or both of the parents is transgender. In 2019 nearly 10% of British babies are born using the IVF procedures pioneered over 40 years ago in 1978. In another 40 years it possible to envisage that a similar proportion of children will have a transgender mother or father, and have been gestated and born using the various medical procedures that are now just being realised.
Examples Warning: Some of the hormone regimes stated below seem to be excessively high, overdosing on hormones will not have any additional physical feminisation effects but does have very serious and dangerous health risks. Hormones should only be prescribed and taken under qualified professional supervision.
More
contributions and information are very welcome, and your identity will
remain confidential unless you consent otherwise. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
(c) 2000 - 2024 Annie Richards
Please send any comments, feedback or additions to:

Last updated: 29 November, 2023

 Notes:
Notes:

























 An important development
in 2011 was that the famous/notorious "Standards
of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming
People" (which very few medical professionals dare not to conform
to) advanced a tiny bit as regards the treatment of young transsexuals in its
An important development
in 2011 was that the famous/notorious "Standards
of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming
People" (which very few medical professionals dare not to conform
to) advanced a tiny bit as regards the treatment of young transsexuals in its


 For a long time the clinic received less than 100 referrals a year,
e.g. in the accounting
year 2009/10 there were 97 referals to the clinic, who all underwent
extensive assessment before any treatment was prescribed. However,
after 2010 the number of referals grew dramatically - in 2016/17 it
passed 2000 and a year later 3000. An interesting development was that
referrals for patients 18 and under has swung from 3:1 assigned male at birth
when the clinic was established, to about 1:2.5 assigned female. This
supports reports that some clinics in Asia were now treating twice as many
FTM as MTF patients, reports which were initially received with great
scepticism.
For a long time the clinic received less than 100 referrals a year,
e.g. in the accounting
year 2009/10 there were 97 referals to the clinic, who all underwent
extensive assessment before any treatment was prescribed. However,
after 2010 the number of referals grew dramatically - in 2016/17 it
passed 2000 and a year later 3000. An interesting development was that
referrals for patients 18 and under has swung from 3:1 assigned male at birth
when the clinic was established, to about 1:2.5 assigned female. This
supports reports that some clinics in Asia were now treating twice as many
FTM as MTF patients, reports which were initially received with great
scepticism.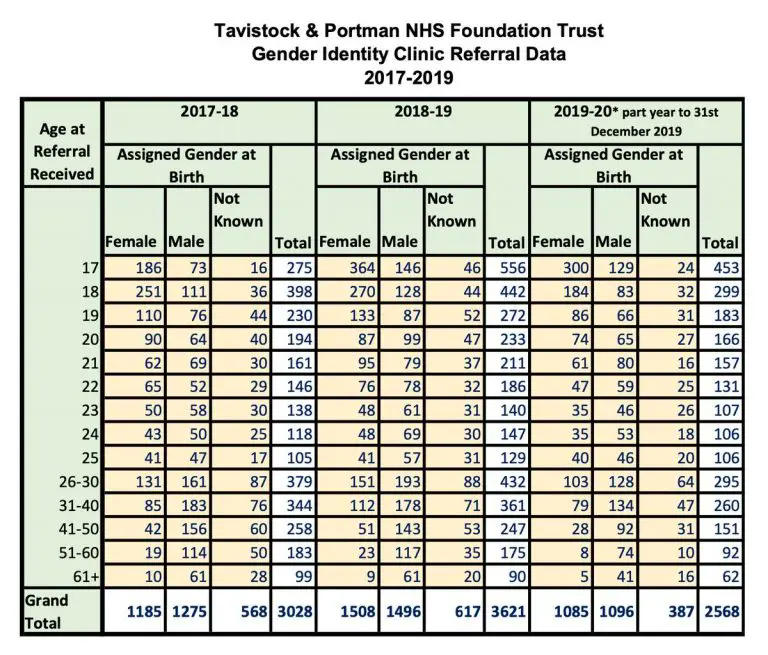









 In the UK transchildren over 16 are legally able to have
gender confirmation surgery with their parents consent. However the
process by which young, trans people access such medical interventions is
subject to additional safeguards and it's unofficially estimated that in
2018 just 35 such procedures were performed privately or via the NHS - a
tiny proportion of the children being identified as having GID.
However, there have been an increasing number of complaints that it has
become to easy for a transgender child to receive irresverable gender
conformatiom surhery.
In the UK transchildren over 16 are legally able to have
gender confirmation surgery with their parents consent. However the
process by which young, trans people access such medical interventions is
subject to additional safeguards and it's unofficially estimated that in
2018 just 35 such procedures were performed privately or via the NHS - a
tiny proportion of the children being identified as having GID.
However, there have been an increasing number of complaints that it has
become to easy for a transgender child to receive irresverable gender
conformatiom surhery. 
















 Final
Note: I would like to give a huge thanks to all the girls who have
contributed to this page in some way.
Final
Note: I would like to give a huge thanks to all the girls who have
contributed to this page in some way.
 Back to Articles
Back to Articles